|
|
 Elon Musk-tweet-26September 2023-Have you heard dis information
|
|
Why Did Zuckerberg Choose Now to Confess?Jeffrey A. Tucker 30August2024 https://brownstone.org/articles/why-did-zuckerberg-choose-now-to-confess/
Consider Mark Zuckerberg’s revelation and its implications for our understanding of the last four years, and what it means for the future.
On many subjects important to public life today, vast numbers of people know the truth, and yet the official channels of information sharing are reluctant to admit it. The Fed admits no fault in inflation and neither do most members of Congress. The food companies don’t admit the harm of the mainstream American diet. The pharmaceutical companies are loath to admit any injury. Media companies deny any bias. So on it goes.
And yet everyone else does know, already and more and more so.
This is why the admission of Facebook’s Mark Zuckerberg was so startling. It’s not what he admitted. We already knew what he revealed. What’s new is that he admitted it. We are simply used to living in a world swimming in lies. It rattles us when a major figure tells us what is true or even partially or slightly true. We almost cannot believe it, and we wonder what the motivation might be.
In his letter to Congressional investigators, he flat-out said what everyone else has been saying for years now.
A few clarifications. The censorship began much earlier than that, from March 2020 at the very least if not earlier. We all experienced it, almost immediately following lockdowns.
After a few weeks, using that platform to get the word out proved impossible. Facebook once made a mistake and let my piece on Woodstock and the 1969 flu go through but they would never make that mistake again. For the most part, every single opponent of the terrible policies was deplatformed at all levels.
The implications are far more significant than the bloodless letter of Zuckerberg suggests. People consistently underestimate the power that Facebook has over the public mind. This was especially true in the 2020 and 2022 election cycles.
The difference in having an article unthrottled much less amplified by Facebook in these years was in the millionfold. When my article went through, I experienced a level of traffic that I had never seen in my career. It was mind-boggling. When the article was shut down some two weeks later – after focused troll accounts alerted Facebook that the algorithms had made a mistake – traffic fell to the usual trickle.
Again, in my entire career of closely following internet traffic patterns, I had never seen anything like this.
Facebook as an information source offers power like we’ve never seen before, especially because so many people, especially among the voting public, believe that the information they are seeing is from their friends and family and sources they trust. The experience of Facebook and other platforms framed the reality that people believed existed outside of themselves.
Every dissident, and every normal person who had some sense that something odd was going on, was made to feel like some sort of crazy cretin who held nutty and probably dangerous views that were completely out of touch with the mainstream.
What does it mean that Zuckerberg now openly admits that he excluded from view anything that contradicted government wishes? It means that any opinions on lockdowns, masks, or vaccine mandates – and all that is associated with that including church and school closures plus vaccine harms – were not part of the public debate.
We had lived through and were living through the most significant far-reaching attacks on our rights and liberties in our lifetimes, or, arguably, on the history record in terms of scale and reach, and it was not part of any serious public debate. Zuckerberg played an enormous role in this.
People like me had come to believe that average people were simply cowards or stupid not to object. Now we know that this might not have been true at all! The people who objected were simply silenced!
During two election cycles, the Covid response was not really in play as a public controversy. This helps account for why. It also means that any candidate who attempted to make this an issue was automatically downgraded in terms of reach.
How many candidates are we talking about here? Considering all the US elections at the federal, state, and local levels, we are talking about several thousand at least. In every case, the candidate who was speaking out about the most egregious attacks on liberty came to be effectively silenced.
A good example is the Minnesota governor’s race in 2022 that was won by Tim Walz, now running as VP with Kamala Harris. The election pitted Walz against a knowledgeable and highly credentialed medical expert, Dr. Scott Jensen, who made the Covid response a campaign issue. Here is how the vote totals lined up.  Tim Walz vote totals Of course, Dr. Jensen could get no traction at all on Facebook, which was enormously influential in this election and which just admitted that it was following government guidelines in censoring posts. In fact, Facebook banned him from advertising completely. It reduced his reach by 90% and likely lost him the election.
You can listen to Jensen’s account here:
 Scott Jensen-tweet-27August2024-IMPOTENT PAWNS
Consider how many other elections were affected. It’s astonishing to think of the implications of this. It means that quite possibly an entire generation of elected leaders in this country was not legitimately elected, if by legitimate we mean a well-informed public that is given a choice concerning the issues that affect their lives.
Zuckerberg’s censorship – and this pertains to Google, Instagram, Microsoft’s LinkedIn, and Twitter 1.0 – denied the public a choice on the central matter of lockdowns, masking, and shot mandates, the very issues that have fundamentally roiled the whole of civilization and set the path of history on a dark course.
And it is not just the US. These are all global companies, meaning that elections in every other country, all over the globe, were similarly affected. It was a global shutdown of all opposition to radical, egregious, unworkable, and deeply damaging policies.
When you think about it this way, this is not just some minor error in judgment. This was an earth-shattering decision that goes way beyond managerial cowardice. It goes beyond even election manipulation. It is an outright coup that overthrew an entire generation of leaders who stood up for freedom and replaced them with a generation of leaders who acquiesced to power exactly at the time it mattered the most.
Why did Zuckerberg choose now to make this announcement and publicly reveal the inside play? He was obviously unnerved by the assassination attempt on Trump’s life, as he said.
Looks like Zuck is trying to say nice things to avoid all responsibility for stealing the election from Trump and censoring all of Trump’s supporters. Zuckerberg belongs in prison. Don’t buy into his bullshit. He’s a conman who is jealous of @elonmusk, And Zuck should rot in prison.  Laura Loomer-tweet-19July2024-Mark Zuckerberg is a conman Then also you have the French arrest of Telegram founder and CEO Pavel Durov, an event which surely rattles any major CEO of a communication platform. You have the arrest and incarceration of other dissidents like Steve Bannon and many others.
You also have the litigation over free speech back in play now that RFK, Jr has been cleared as having standing, kicking the case of Missouri v. Biden back to the Supreme Court, which wrongly decided last time to deny standing to other plaintiffs.
Zuckerberg of all people knows the stakes. He understands the implications and the scale of the problem, as well as the depths of the corruption and deception at play in the US, EU, UK, and all over the world. He may figure that everything is going to come out at some point, so he might as well get ahead of the curve.
Of all the companies in the world that would have a real handle on the state of public opinion right now, it would be Facebook. They see the scale of the support for Trump. And Trump has said on multiple occasions, including in a new book coming out in early September, that he believes Zuckerberg should be prosecuted for his role in manipulating election outcomes. What if, for example, his own internal data is showing 10 to 1 support for Trump over Kamala, completely contradicting the polls which are not credible anyway? That alone could account for his change of heart.
It becomes especially pressing since the person who did the censoring at the Biden White House, Rob Flaherty, now serves as Digital Communications Strategist for the Harris/Walz campaign. There can be no question that the DNC intends to deploy all the same tools, many times over and far more powerful, should they take back the White House.  Rob Flaherty letter “Under Rob’s leadership,” said Biden upon Flaherty’s resignation, “we’ve built the largest Office of Digital Strategy in history and, with it, a digital strategy and culture that brought people together instead of dividing them.”
At this point, it’s safe to assume that even the most well-informed outsider knows about 0.5% of the whole of the manipulation, deception, and backroom machinations that have taken place over the past five or so years. Investigators on the case have said that there are hundreds of thousands of pages of evidence that are not classified but have yet to be revealed to the public. Maybe all of this will pour forth starting in the new year.
Therefore, the Zuckerberg admission has much larger implications than anyone has yet admitted. It provides a first official and confirmed peek into the greatest scandal of our times, the global silencing of critics at all levels of society, resulting in manipulating election outcomes, a distorted public culture, the marginalization of dissent, the overriding of all free speech protections, and gaslighting as a way of life of government in our times. Author |
|
Jury: Bay Area Transit Workers Fired for Refusing COVID-19 Vaccine to Get More Than $1 Million EachAt issue is a vaccine mandate for BART workers in San Francisco that was imposed in 2021.By Jack Phillips
Rail transit officials in California’s Bay Area have been ordered to pay more than $7 million to transit workers who were fired because they refused to get a COVID-19 vaccine years ago.
On Oct. 23, a federal jury in the U.S. District Court for the Northern District of California sided with six former San Francisco Bay Area Rapid Transit (BART) workers who had refused to get the vaccine for religious purposes.
BART was ordered to pay the group more than $7.8 million, with each individual receiving between $1.2 million and $1.5 million, the Pacific Justice Institute, which represented the transit workers in the trial, said in a statement on Oct. 24. The institute, a law firm representing the six former employees since 2022, said the eight-person jury deliberated for two days this week before returning the verdict that awarded the employees the compensation.
About a week ago, the federal jury also determined that BART had failed to prove that it suffered an undue hardship by denying accommodations to the ex-employees in the case.
On Oct. 23, the jury further found that the six employees met the burden of showing that there was a conflict between their religious beliefs and the BART vaccine mandate, which was implemented in 2021.
According to the law firm, the jury also agreed with the figures that the plaintiffs had provided for lost wages that they had suffered after losing their jobs. The jury then added $1 million each to those figures, the firm said, describing the verdict as a “legal earthquake.”
“The rail employees chose to lose their livelihood rather than deny their faith. That in itself shows the sincerity and depth of their convictions,“ Kevin Snider, the Pacific Justice Institute’s chief counsel, who served as lead trial attorney, said. ”After nearly three years of struggle, these essential workers feel they were heard and understood by the jury and are overjoyed and relieved by the verdict.”
The law firm stated: “During the trial, jurors heard compelling testimony from dedicated employees. One of the plaintiffs had worked for more than 30 years for BART, with a stretch of 10 years perfect attendance, before being unceremoniously dismissed. Another had been out on workers comp for months, with no scheduled return date, when she was fired.”
Lawyers for BART argued that multiple employees who had conflicts with receiving the vaccine had secular—rather than religious—reasons. But the jury disagreed with those arguments, the Pacific Justice Institute said.
The vaccine mandate was approved by BART’s board of directors in October 2021 and stipulated that all employees must get the COVID-19 vaccine. It allowed some employees to be exempt from the vaccine, including for religious reasons.
A year later, BART employees filed a class-action lawsuit accusing the operator of denying religious accommodations in violation of state law.
U.S. District Judge William Alsup, who presided over the lawsuit against BART, ruled that the operator’s policies did not violate the employees’ right to religious freedom, according to an order he issued in March.
A separate order issued by Alsup in January found that BART received 188 requests for a religious exemption and accommodation, and of that figure, 40 chose not to complete the process. They were either terminated from employment or ultimately got the vaccine.
“Plaintiffs’ putative class fails because its members have little in common beyond their request for religious accommodation,” the judge further said in his order. “They do not share a common religious objection. They do not share a vocation or a set of contractual rights. They do not present a similar set of potential accommodations and associated burdens. They do not present similar health and exposure concerns.
“Potential accommodations do not impact the same pool of coworkers. Those coworkers do not have the same bargained-for rights.”
The Epoch Times contacted BART for comment on Oct. 25 but received no reply by publication time. The rail operator’s spokesman, James Allison, told local news outlet SFGate that it had “no comment” on the verdict.
|
|
Federal Court Rules Against FDA Over Anti-Ivermectin PostsBy Zachary Stieber
The U.S. Food and Drug Administration (FDA) likely overstepped its authority when it told Americans to “stop” using ivermectin against COVID-19, a federal court ruled on Sept. 1.
“FDA can inform, but it has identified no authority allowing it to recommend consumers ‘stop’ taking medicine,” U.S. Circuit Judge Don Willett wrote in the ruling.
The FDA has authority under the Federal Food, Drug, and Cosmetic Act to convey information to consumers. The FDA during the COVID-19 pandemic has issued multiple statements discouraging people from taking ivermectin against COVID-19.
Accompanied by a picture of a horse and a link to an FDA webpage on ivermectin, the agency wrote in one social media post: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
The page it linked to is titled, “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19.”
Three doctors sued the FDA over its statements on ivermectin, arguing the agency cannot advise doctors on which drugs to prescribe.
Ivermectin is approved by the agency as an antiparasitic drug for both humans and animals. Federal law gives the government immunity against legal actions, with some exceptions. One exception, known as ultra vires, is when an official acts outside their authority. Plaintiffs challenging the acts must show that the official was “acting ‘without any authority whatever,’ or without any ‘colorable basis for the exercise of authority,'” according to an earlier court ruling.
The FDA does have the authority to share data and facts, the parties agree. But they diverge on whether the FDA can issue recommendations on medical matters, such as treatments.
The FDA has claimed that the posts do not contain advice, stating in one brief that they were “informational statements” that “do not ‘direct’ consumers, or anyone else, to do or refrain from doing anything.” At the same time, the FDA acknowledged that the statements “provided recommendations” and “advise[d] consumers.”
“Despite these concessions, FDA never points to any authority that allows it to issue recommendations or give medical advice,” Judge Willett wrote.
“Rather, FDA argues that some posts included a hyperlink that leads to the update. The update, in turn, directs consumers to “[t]alk to your health care provider.” But not all of the social-media posts included such a link. And even for those posts that did include a link, the posts themselves offer advice, not mere information.”
The update itself is problematic because of its title, “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19,” the judge said. Even though it later says that people can take ivermectin if prescribed by a health care provider, “the trailing qualifier does not lessen the opening instruction’s imperative character,” he said. Exposing the FDA’s Orwellian Lie About Ivermectin | CLIP | Facts MatterU.S. District Judge Jeffrey Brown ruled against the doctors in 2022, finding that doctors had not proven an exception to sovereign immunity and that there was no indication the FDA acted outside of the authority conferred by the Federal Food, Drug, and Cosmetic Act. Judge Brown erred on the second point as well, according to the new ruling. “Nothing in the Act’s plain text authorizes FDA to issue medical advice or recommendations,” Judge Willett said. The judge, who sits on the U.S. Court of Appeals for the Fifth Circuit, was joined by U.S. Circuit Judges Edith Brown Clement and Jennifer Walker Elrod.
Judges Willett and Brown were appointed under President Donald Trump. Judges Clement and Elrod were appointed under President George W. Bush.
The appeals court panel remanded the case back to Judge Brown to decide on whether the doctors have standing. The ruling followed oral arguments before the panel.
Dr. Robert Apter, one of the plaintiffs, called the ruling “a big win for doctors and for patients!” “This case has broad implications for protecting the practice of medicine from unlawful interference by the FDA,” added Jared Kelson, a lawyer at Boyden Gray who is representing the plaintiffs. “It’s about ensuring that federal agencies act only within their statutory authority. The FDA crossed a bright line here.” The U.S. government has not yet reacted to the ruling.
Zachary Stieber Zachary Stieber is a senior reporter for The Epoch Times based in Maryland. He covers U.S. and world news. |
|
Doctor: Pharmacists Continuing to Refuse Ivermectin Prescriptions, Raising Ethical ConcernsCOVID Treatments & Remedies
The continued refusal of pharmacists nationwide to fill prescriptions for controversial COVID medications has raised questions over medical autonomy and who ultimately has control over patient care, according to a prominent doctor.
Dr. Mary Talley Bowden, a practitioner and founder of Coalition of Health Freedom, told The Epoch Times that many pharmacists nationwide are still refusing to fill prescriptions issued for ivermectin issued to patients for the treatment of COVID, despite statements from the Food and Drug Administration (FDA) affirming that right to doctors.
“This needs to come to an end. In telling my patients what medicines they can and cannot have access to, we effectively have a large group of pharmacists practicing medicine without a license,” said Dr. Bowden. “They have no accountability for this yet they are allowed to dictate patient care.”
“I see it every single day. Enough is enough,” Dr. Bowden added. Ivermectin has been around for decades but became the center of controversy in 2020 after medical opinion became divided over its effectiveness as a treatment for COVID. In the aftermath, many pharmacists refused to fill prescriptions for the medication.
By 2023, the issue had made its way into a courtroom when on Aug. 8 a lawyer representing the FDA confirmed that doctors were free to prescribe ivermectin to treat COVID.
“FDA explicitly recognizes that doctors do have the authority to prescribe ivermectin to treat COVID,” Ashley Cheung Honold, a Department of Justice lawyer representing the FDA, told the U.S. Court of Appeals for the 5th Circuit.
The government lawyer made the statement in defense of the FDA’s repeated calls for people to not take ivermectin for COVID. The FDA on Aug. 21, 2021, wrote on X, formerly known as Twitter: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
On Aug. 17, the FDA issued clarification, this time stating that while it had approved ivermectin for certain uses in humans and animals, it had not issued any statement affirming the safety or effectiveness of the drug for treating COVID. However, the agency again affirmed that it would be left to individual doctors whether or not to prescribe the medication for the treatment of COVID.
“Health care professionals generally may choose to prescribe an approved human drug for an unapproved use when they judge that the unapproved use is medically appropriate for an individual patient,” the FDA said.
The National Institutes of Health COVID-19 treatment guidelines recommend against using ivermectin for COVID treatment, citing a purported lack of evidence supporting its effectiveness. Other studies have found ivermectin to be effective.
Dr. Bowden, who is one of three plaintiffs in the case, had hoped the FDA’s acknowledgment would have put an end to the objections at the pharmacist counter. However, earlier this week another one of her patients who she had been treating was refused service. Complicating the situation, the patient was elderly and couldn’t easily access other options and in the time it took to find a pharmacy that would honor the prescription the patient’s health began to deteriorate, according to Dr. Bowden.
“It’s hard to believe, but pharmacists are still blocking these potentially life-saving medications,” said Dr. Bowden. “The pharmacist didn’t talk to the patient and won’t know if the patient lives or dies yet had control of his care.”
Dr. Bowden believes that in most cases individual pharmacists aren’t the ones to blame, and are often carrying out orders from corporate leadership. However, claims to have seen examples where pharmacists prevented her patients from getting their medication as a result of their own “personal agenda.”
“It’s an outrage. I would have thought we were beyond this but it continues to happen,” said Dr. Bowden. If this newfound power isn’t checked, it could lead down a slippery slope that diminishes patient’s rights, according to Dr. Bowden.
“Prior to COVID, I never had a pharmacist refuse a prescription. This is a new phenomenon and it needs to come to an end. This is going beyond their role and it’s a dangerous trend,” said Dr. Bowden.
Sen. Ron Johnson (R-Wis.), believes that the widespread denial of ivermectin could have resulted in untold COVID deaths. “The doctors I’ve been dealing with and talking to for years now, they believe that probably hundreds of thousands of Americans lost their lives because they were denied early treatment and they were denied because the FDA sabotaged, for example, ivermectin,” Mr. Johnson told FOX News on Aug. 11.
“We are going down a very dangerous path, but it’s a path that is being laid out and planned by an elite group of people that want to take total control over our lives, and that’s what they’re doing bit by bit,” he added. |
|
‘FDA Is Not a Physician’: Appeals Court Sides With Doctors on Ivermectin for COVID-19COVID Treatments & Remedies
A federal appeals court in New Orleans ruled on Friday that the Food and Drug Administration (FDA) had overstepped its authority in their ruling that three doctors will be able to move forward with their lawsuit over the use of ivermectin off-label to treat COVID-19.
Dr. Mary Talley Bowden, one of three doctors who initially filed the petition, trumpeted the ruling as a victory for not only the truth, but patient rights.
“The FDA misled the public into thinking it has more authority than it does,” Dr. Bowden, a practitioner and founder of Coalition of Health Freedom, told The Epoch Times. “This decision confirms that the FDA is not your doctor and has no authority to tell doctors how to practice medicine.”
Judge Don Willett wrote for the three person panel that also included Jennifer Walker Elrod and Edith Brown Clement. “The Doctors have plausibly alleged that FDA’s Posts fell on the wrong side of the line between telling about and telling to.”
“FDA is not a physician. It has authority to inform, announce, and apprise—but not to endorse, denounce, or advise. The Doctors have plausibly alleged that FDA’s Posts fell on the wrong side of the line between telling about and telling to. As such, the Doctors can use the APA to assert their ultra vires claims against the Agencies and the Officials.”
The anti-ivermectin messaging put out by FDA officials also drew the ire of Judge Willett, who wrote that “Left unmentioned in most of that messaging: ivermectin also comes in a human version. And while the human version of ivermectin is not FDA-approved to treat the coronavirus, some people were using it off-label for that purpose.”
In the ruling social media posts made by the agency were cited as evidence, citing that “Even tweet-sized doses of personalized medical advice are beyond FDA’s statutory authority,” he wrote.
The FDA on Aug. 21, 2021, wrote on X, formerly known as Twitter: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.”
The National Institutes of Health COVID treatment guidelines recommend against using ivermectin for COVID treatment, citing a purported lack of evidence supporting its effectiveness. Other studies have found ivermectin to be effective.
The lawsuit was initially filed in June 2022 by Dr. Bowden, Drs. Robert L. Apter, and Paul E. Marik for interfering with both their authority to prescribe an approved medication and the doctor-patient relationship. All three alleged their reputations were harmed by the FDA campaign. Dr. Bowden lost admitting privileges at a Texas hospital while Dr. Marik alleged he lost his jobs at a medical school and at a hospital for promoting the use of ivermectin.
The ruling comes as a blow to the FDA. The agency had argued that the case should not be allowed to move forward, claiming that the complaints didn’t overcome the FDA’s “sovereign immunity,” which protects government entities from many civil lawsuits regarding their responsibilities.
The FDA did not immediately respond to requests for comment. The refusal of pharmacists nationwide to fill prescriptions for ivermectin has become a hot-button issue, raising questions over medical autonomy and who ultimately has control over patient care.
Ivermectin has been around for decades but became the center of controversy in 2020 after medical opinion became divided over its effectiveness as a treatment for COVID. In the aftermath, many pharmacists refused to fill prescriptions for the medication.
On Aug. 8 a lawyer representing the FDA confirmed that doctors were allowed to prescribe ivermectin to treat COVID. “FDA explicitly recognizes that doctors do have the authority to prescribe ivermectin to treat COVID,” Ashley Cheung Honold, a Department of Justice lawyer representing the FDA, told the U.S. Court of Appeals for the 5th Circuit.
FDA Detects Serious Safety Signal for Covid Vaccine Among KidsDr. Bowden claims that despite the endorsement from the FDA, the practice of pharmacists refusing to fill prescriptions for ivermectin continues.
“This needs to come to an end. In telling my patients what medicines they can and cannot have access to, we effectively have a large group of pharmacists practicing medicine without a license,” said Dr. Bowden told the Epoch Times on Friday. “They have no accountability for this yet they are allowed to dictate patient care.”
“I see it every single day. Enough is enough,” Dr. Bowden added.
|
|
FDA loses its war on ivermectin and agrees to remove all social media posts and consumer directives
This landmark case sets an important precedent in limiting FDA overreach into the doctor-patient relationship. Thank you @BoydenGrayPLLC for your excellent counsel. @drpaulmarik1 @RobertApter1 @Covid19Critical  Mary Talley Bowden MD-tweet-22March2024-FDA loses its war on ivermectin
|
|
FDA Has ‘Gone Rogue’ in Its Approval of New COVID-19 Boosters: Dr. Robert MaloneDr. Malone accused the FDA of flouting its own rules and “going rogue” by green-lighting updated COVID-19 vaccines with limited clinical trial data. Dr. Peter McCullough, a cardiologist, speaks at the Conservative Political Action Conference at the Hilton Anatole in Dallas on Aug. 5, 2022. (Bobby Sanchez/The Epoch Times) By Tom Ozimek and Joshua Philipp The Food and Drug Administration (FDA) has “gone rogue,” according to virologist Dr. Robert Malone, who accused the federal agency of sacrificing its own rules and regulations with its decision to recommend the latest batch of COVID-19 boosters, which only have limited clinical trial data attesting to their efficacy and safety.
Dr. Malone made the remarks in an interview with EpochTV’s “Crossroads” program on Sept. 11, the day that the FDA cleared new COVID-19 vaccines in a bid to counter the waning effectiveness of the currently available shots.
“It’s difficult to conclude anything other than the FDA is no longer feeling bound by their own rules and regulations,” Dr. Malone said. “The term is—they’ve gone rogue.”
Dr. Malone said the lack of human clinical trial data demonstrating effectiveness and safety of the updated vaccines should have precluded their approval by the FDA.
He said that, essentially, the FDA authorized the new vaccines on the premise that “neutralizing antibodies as detected in mice and their cross-reactivity are correlative protection,” which he said “is a lie, there are no established correlates of protection for SARS-CoV-2.” FDA officials didn’t respond by press time to a request by The Epoch Times for comment.
The agency cleared Moderna’s and Pfizer’s newest mRNA vaccines on Sept. 11 without analyzing data from any human trials.
In a statement announcing its approval, the FDA said that the decision was supported by its evaluation of “manufacturing data” from vaccine producers and “non-clinical immune response data on the updated formulations including the XBB.1.5 component.”
The benefit-risk profile of earlier versions of the vaccines is “well understood,” the FDA claimed, adding that the similar manufacturing process for the updated vaccines “suggests that the vaccines are a good match for protecting against the currently circulating COVID-19 variants.”
The Centers for Disease Control and Prevention (CDC) followed with its own recommendation on Sept. 12, urging nearly all Americans to get the new vaccines. The shots will be available to children as young as 6 months old this month. Dr. Robert Malone: The Coordinated Propaganda Narrative Around COVID-19 | CLIP
The new vaccines target XBB.1.5, a sub-type of the Omicron variant of the SARS-CoV-2 virus, which causes the disease COVID-19. However, the XBB.1.5. subvariant has already largely been displaced by newer strains of the quickly evolving virus, including EG.5, according to the CDC.
While FDA documents show the agency did not include any trial data in its review of the new shots, data from a Moderna trial was considered by the CDC before it issued its recommendation. The trial featured just 50 people receiving a new shot, and found the vaccine induced levels of neutralizing antibodies that authorities said would protect against COVID-19. One of the 50 people suffered a vaccine-related adverse reaction.  Florida Surgeon General Dr. Joseph Ladapo in Tampa, Fla., on Oct. 15, 2022. (York Du/The Epoch Times)
‘Lot of Red Flags’“There’s essentially no data,” Florida Surgeon General Dr. Joseph Ladapo said at a recent news conference, where he suggested that people might be better off passing on the new round of shots.
“Not only that, but there are a lot of red flags,” Dr. Ladapo added, while pointing to studies finding that the effectiveness of the vaccines turns negative over time.
“There’s been no clinical trial done in human beings showing that it benefits people, there’s been no clinical trial showing that it is a safe product for people.”
He also noted that studies have linked previous versions of the COVID-19 vaccine to cardiac problems such as heart inflammation.
“It’s truly irresponsible for FDA, CDC, and others to be championing something … when we don’t know the implications of it,” Dr. Ladapo said.
Asked to comment on Dr. Ladopo’s remarks, Dr. Malone pointed to a growing body of studies that show negative vaccine effectiveness, which he said suggests that, in the risk-benefit analysis, “there’s no discernible benefit, or there’s negative benefit, but there’s clearly risk.” ‘Most Americans Take Them’While acknowledging the current vaccines’ waning effectiveness, CDC Director Mandy Cohen penned an op-ed in The New York Times on Sept. 13, in which she called the updated COVID-19 vaccines “one of the most effective tools in combating the virus.”
“Covid-19 vaccines are the best way to give the body the ability to keep the virus from causing significant harm. Extensive studies and real-world experience have shown that they are safe and they work,” she wrote. “And most Americans take them.”
Dr. Cohen said the vaccines were put through extensive clinical trials before they were introduced in 2021 and “since then, their safety has been intensely monitored.”
She didn’t address criticism, such as the little trial data that’s been made available.
That FDA and CDC moves have been questioned by a number of doctors. Dr. Paul Offit, an FDA adviser, suggested to the UK’s Daily Mail that younger, healthy people who have already been vaccinated don’t need one of the new doses.
“We are best served by targeting these booster doses to those who are most at risk of severe disease,” such as people older than 75, Dr. Offit said. “Boosting otherwise healthy young people is a low-risk, low-reward strategy.”
In his remarks at the news conference, Dr. Ladapo asked people to make decisions based on their “resonance of truth” rather than depending on “very educated people telling you what you should think.”
“When they try to convince you to be comfortable and agree with things that don’t feel comfortable and don’t feel like things you should agree with, that’s a sign … And I encourage you and certainly beg and hope that you do listen to it, because it will serve you right,” he said.
A January–July 2023 study that analyzed data from 33 California state prisons found that individuals who received new COVID-19 booster shots were more likely to contract COVID-19 compared to those who didn’t receive the jabs.
The infection rate among the group that received the bivalent booster shots came in at 3.2 percent—higher than the 2.7 percent among the unvaccinated.
Late last month, the CDC conceded that the new BA.2.86 strain can cause infection even among people who have previously been vaccinated against COVID-19.
“The large number of mutations in this variant raises concerns of greater escape from existing immunity from vaccines and previous infections compared with other recent variants,” the agency said in its assessment.
Zachary Stieber contributed to this report.
|
|
British Court Rules That Competent & Conscious Patient Can Be Denied Life-Sustaining Treatment Against Her Willby Tyler Durden, 04September2023 – https://www.zerohedge.com/medical/british-court-rules-competent-conscious-patient-can-be-denied-life-sustaining-treatment In my torts class, I often compare the different approaches and doctrines in the United States and the United Kingdom. One of the most pronounced is the position and authority of physicians on issues like consent and malpractice. This week produced a particularly striking example.
British doctors are seeking to take a 19-year-old critically ill female patient off the intensive care despite her objections and those of her parents.
Unlike most such cases, the woman known only as “ST” is conscious and communicative. Yet, the doctors argue that she is not being realistic about her chances of survival from a rare disorder. Now a British court has agreed and ordered that she can be placed on end-of-life care against her will. ST is suffering from a rare genetic mitochondrial disease that is progressively degenerative. The case has similarities to that of Charlie Gard, an infant who was removed from life support at the insistence of doctors despite objections from the parents. The Gard family was seeking to take Charlie to the United States for experimental treatment.
ST has been in the ICU for the past year, requiring a ventilator and a feeding tube. She also requires regular dialysis due to chronic kidney damage from her disease. She wants to be allowed to travel to Canada for an experimental treatment but the doctors oppose the plan and say that she is not accepting the realities of her terminal illness. They say that she is “actively dying” without any hope of resuming life outside of intensive care. Her deeply religious family have spent their entire life savings on her care and has complained that a “transparency order” requested by the hospital barred their ability to give details on the case to help raise public funds.
What is so remarkable about this case is that it is not an infant or a comatose patient. The court found that ST “is able to communicate reasonably well with her doctors with assistance from her mother and, on occasion, speech therapists.”
Moreover, two psychiatrists testified that she is mentally competent to make decisions about her own care.
Nevertheless, the judge found that she is mentally incapable of making decisions for herself because “she does not believe the information she has been given by her doctors.”
The court appears to reject her ability to make this decision because she is making the wrong decision:
Accordingly, the court ruled that decisions about ST’s further care should be determined by the Court of Protection based on an assessment of her best interests. Her “best interest,” according to the doctors, is to die. Thus, the courts have declared that ST cannot choose to continue life-extending treatment and can be forced into palliative care against her will. The logic of the decision is chilling.The court is told that ST has cognitive and communicative abilities to make such decisions. However, because the court disagrees with her desire to continue to fight to live, she is treated as effectively incompetent. It seems like the judicial version of Henry Ford’s promise that customers could pick any color car so long as it is black. Here is the opinion: In the Matter of ST
|
|
Higher Incidence of COVID-19 Found Among Consistent Mask-Wearers: StudySome mask wearers were found to have up to 40 percent higher incidence of infection, contradicting earlier studies and opposing the narrative of mask mandates.By Naveen Athrappully 27November2023 Updated: 29November2023 https://www.theepochtimes.com/health/study-finds-higher-incidence-of-covid-19-among-consistent-mask-wearers-5536488
People who wore protective masks were found to be more likely to contract COVID-19 infections than those who didn’t, according to a recent Norwegian study.
The peer-reviewed study, published in the journal Epidemiology and Infection on Nov. 13, analyzed mask use among 3,209 individuals from Norway. Researchers followed them for 17 days, and then asked the participants about their use of masks. The team found that there was a higher incidence of testing positive for COVID-19 among people who used masks more frequently.
Among individuals who “never or almost never” wore masks, 8.6 percent tested positive. That rose to 15 percent among participants who “sometimes” used masks, and to 15.1 percent among those who “almost always or always” wore them.
Adjusting for factors such as vaccination status, the study determined that individuals who sometimes or often wore masks had a 33 percent higher incidence of COVID-19, compared to those who never or almost never wore masks. This jumped to 40 percent among people who almost always or always wore them.
However, adjusting for “differences in baseline risk over time,” the risk of wearing masks turned out to be “less pronounced,” with only a 4 percent higher incidence of infection among mask-wearers.
“The results contradict earlier randomized and non-randomized studies of the effectiveness of mask-wearing on the risk of infection,” the researchers wrote.
“Most of these studies reported that wearing a face mask reduces the risk of COVID-19 infection. Some observational studies have reported manyfold reductions while one community-based randomized trial failed to demonstrate a statistically significant reduction in infection risk and one cluster randomized community trial found only a modest reduction.”
The researchers pointed out a major limitation of their study: Individuals who used masks may have done so to protect others from their own infection. This could explain the “positive association between risk of infection and mask usage.”
Behavioral differences and the fact that the survey was based on self-reporting could also contribute to bias, it stated. There’s also a possibility that mask wearers felt safe while wearing masks and thus didn’t follow other regulations such as social distancing, which raised their risk of contracting COVID-19, the study said.
“Our findings suggest that wearing a face mask may be associated with an increased risk of infection. However, it is important to note that this association may be due to unobservable and non-adjustable differences between those wearing and not wearing a mask,” the researchers stated.
“Therefore, caution is imperative when interpreting the results from this and other observational studies on the relationship between mask-wearing and infection risk. Recommendations to wear face masks in the community are largely informed by low certainty evidence from observational studies.”
Researchers called for more trials and studies to gain a better understanding of the effectiveness of wearing masks against transmission of respiratory pathogens.
The study was fully funded by the Norwegian Institute of Public Health. It reported no conflicts of interest. Masking MandatesThe new study comes at a time when some regions in North America are reinstating mask mandates amid a reported increase in COVID-19 cases.
At the beginning of November, many regions in the Bay Area issued masking rules in health care settings ahead of the respiratory disease season, when infections such as COVID-19, the flu, and respiratory syncytial virus are expected to spread. In the state of California, San Francisco, Alameda, Santa Clara, San Mateo, Marin, Contra Costa, Napa, Sonoma, and Solano issued masking mandates, with the rules remaining in effect until next March or April.
While in some places only staff and workers of a health care facility are required to wear masks, others require patients and visitors to wear masks as well. Rosemary Hills School in Maryland announced in September that it distributed KN95 masks to students and teachers while mandating masking for at least 10 days after three students from a classroom tested positive for COVID-19.
A month earlier, school officials with the Kinterbish Junior High School in Cuba, Alabama, asked students, employees, and visitors to wear masks “due to the slow rise of COVID cases in the area.”
Seven hospitals in Canada reinstated mask mandates last month to “help prevent transmission of COVID-19.”
In British Columbia, Provincial Health Officer Bonnie Henry announced that health care workers, volunteers, and visitors would be required to wear “medical” masks in all public health care facilities starting on Oct. 3.
The Centers for Disease Control and Prevention recommends wearing masks to counter COVID-19. “Masking is a critical public health tool and it is important to remember that any mask is better than no mask,” it said in an August 2021 update.
Certain states have already made it clear that mask mandates wouldn’t be allowed. In August, Texas Gov. Greg Abbott said in an X post that there would be “NO mask mandates in Texas.” Florida Surgeon General Joseph Ladapo highlighted the issue of the ineffectiveness of masking policies.
“What do you call re-imposing mask policies that have been proven ineffective or restarting lockdowns that are known to cause harm? You don’t call it sanity,” he said in a post on X. “These terrible policies only work with your cooperation. How about refusing to participate.”
Several studies have questioned the use of masks to prevent viral transmission. A review published in late January at the Cochrane Library that analyzed 78 randomized controlled trials found that they didn’t show “a clear reduction in respiratory viral infection with the use of medical/surgical masks.”
In an interview with the Brownstone Institute in February, Tom Jefferson, a senior associate tutor at the University of Oxford and lead author of the study, pointed out that there hasn’t been a “proper trial” of masks whereby a huge, randomized study was done to check their effectiveness. Instead, some experts overnight began to perpetuate a “fear-demic.”
|
|
What Some Call “Anti-Science” Is Just Anti-Authoritarianismby Tyler Durden, 20october2023 – https://www.zerohedge.com/political/what-some-call-anti-science-just-anti-authoritarianism Authored by Alex Washburne via The Brownstone Institute,
 What is up, What is down? Sometimes it feels as if we’re living in a dizzying house of narrative mirrors and anyone sincerely interested in walking the true path through the world risks being unable to see the true path as they get trapped in our horrific hall of insincere reflections.
The truth of any given matter, the objective facts and consilient theories, seems to matter less than the ability of an idea or narrative to reflect back to people what they wish to see. Our marketplace of ideas incentivizes manufacturing narrative mirrors that provide epistemological narcissists an opportunity to view themselves in a favorable light and secure a foothold in media outlets that have devolved from curators of our frontal lobe to antagonists of our amygdala.
Speaking of epistemological narcissists and narrative mirrors, let’s talk about Peter Hotez and his narrative of a growing “Anti-Science” movement.
Peter Hotez self-identifies as a scientist and appears to spend most of his time running around predominately liberal media outlets, using his stature as “The Scientist” to misrepresent, demean, and cry “disinformation” on information, worldviews, and even scientific theories that differ from his own. Any scientist who disagrees with Dr. Hotez and his outrageous, inhuman, insensitive, and irrational proclamations is blocked and ridiculed. While truth may bounce off Hotez like bullets off of Thanos, it appears our disagreements have successfully penetrated the armor of Dr. Hotez’s ego and a new ego-defense is materializing.
Now, Dr. Hotez claims that there is “an Anti-Science movement,” a cultural and political boogeyman that is out to undermine science and target scientists. I have little doubt he would love to snap his fingers and make what he views as “Anti-Science” people, beliefs, and institutions disappear in an act of anti-heroic benevolence for the world.
The whole notion of “Anti-Science,” however, is a narrative. It is not a physical object like “anti-matter” or “antigen” nor is it a process like “antibody maturation” nor an objective and diagnosable clinical condition like “antisocial personality disorder.” “Anti-Science” is nothing but an attempt to name a thing that Hotez sees, but he views our political world from a far-off silo and lives in a hall of mirrors of his own design. As a consequence of Hotez’ distance from the people and patterns he’s labeling “Anti-Science,” the thing he sees is not a thing that exists in our shared, objective universe.
To understand what Hotez sees, why he sees it, and why it’s not a thing in our universe, we have to provide, to the best of our ability, a minimal and objective set of historical facts that can reproduce what he sees. I hypothesize one can synthesize Hotez’ toxic worldview by following the 7-step recipe below:
If these seven criteria are met, I believe someone like Peter Hotez will be a nearly inevitable social consequence. The simple explanation is that the criteria above polarized scientists (1) without them knowing they are polarized (2), gave them an opportunity (3) to exercise somewhat unchecked State power (4), and gave them media power (5) to suppress dissent by calling it “disinformation” (6).
The first six steps of this recipe create an authoritarian ethos in scientists – Trust the Science, Follow the Science – and compel them to act on these politically ethnocentric and authoritarian impulses with few checks and balances except for popular discontent. Inevitably, the siloed and politically biased composition of scientists will result in policies that sow massive discontent (lockdowns, mask mandates, vaccine mandates). When we add the 7th ingredient of the recipe, people exposed to an authoritarian bunch of scientists brushing aside their humanity, their political rights, and their distinct value systems will express their discontent. The people expressing discontent will correctly identify the scientists as the people and groups of scientists as the syndicate that corrupted the public policy process through unfair, undemocratic, and intolerant tactics, and the people will speak their minds at these scientists – like Hotez – in public fora.  Boston Tea Party From Wikipedia
The Hotez’s will need to be fermented in this social and media concoction of authoritarianism within grasp hindered by legitimate public criticism for some time. Eventually, they will need a narrative to brush away that public resistance so they will create an ego-defensive narrative that positions them as heroes, Scientists as Saviors (scientific saviorism). Hotez and others have somewhat of a manic pixie dream scientist view of themselves – the scientists who are apolitical heroes of infinite cultural latitude exist only in their imaginations to serve their fantasies of grandiosity and benevolence. They sincerely believe that if science says X is effective at reducing one disease then all of society ought to Follow the Science to adopt X, mandate X, do whatever it takes to make X ubiquitous and thank scientists for X. Of course, the tricky thing about society is that it is comprised of humans, a vast anthropological mosaic of beliefs and value systems, and there are other beliefs and value systems that believe we ought to do Y.
Science has become a central pillar of the Saviors’ self-identity and so they don’t distinguish between science (the objective and often messy process of fairly evaluating many competing ideas) and the authoritarian actions of scientists. As the Toxic Hotez nears completion from cooking in a vat of legitimate public criticism for their scientific ethnocentrism, they will conceive a global conspiracy targeting science and scientists, a monstrous “Anti-Science” that demands even more power and legal protection of scientists, even stronger measures to police disinformation. As they look at the restored image of Scientists as Saviors in this narrative mirror, they will descend even further into madness.
Indeed, it is madness because what Hotez views as “Anti-Science” does not exist, it is not a good reflection of reality but rather a story told from pride and ego-defense. Hotez, a set of scientists closely connected with the heads of the NIH, NIAID, and other global health science funders (none of them democratically elected), and even the funders themselves ate the forbidden fruit of authoritarianism. Many before Hotez have tasted authoritarianism, and the results are predictable. The Scientists who grabbed the reigns of society during the pandemic and steered it with insensitive ambition are experiencing not a novel monstrosity but an age-old and dignified human response called “Anti-Authoritarianism.” Some – not all – scientists acted like authoritarians during the COVID-19 pandemic.Some – not all – scientists rallied around models from the most powerful and well-funded scientific groups at the start of the pandemic, even if their models were clearly wrong. When some scientists like John Ioannidis spoke up about the shortcomings of models that were guiding policy, the politically siloed scientists reacted with vitriol and social power that could crush careers in scientific institutions. The informal social control of scientists suppressed diverse views and resulted in science not shared.
So some – not all – scientists became very vocal in advocating for lockdowns despite the policy being inhumane and a clear violation of civil liberties, such as when fellow scientists Jay Bhattacharya, Martin Kulldorff, and Sunetra Gupta wrote the Great Barrington Declaration (GBD) arguing that lockdowns were likely to cause harm and that all-cause mortality and morbidity could be reduced by focusing our protection and helping those with high risk of severe outcomes receive the best preventative support and treatment we could muster. The GBD was an alternative policy proposal that was also grounded in science and it differed in its moral calculus and focus on all-cause mortality. The GBD was assisted by a group whose beliefs aligned with the policies and ideas therein – the American Institute for Economic Research. That group was said to be a libertarian think tank.
There was just two problems with the Great Barrington Declaration: it was supposedly aligned with a group whose political preferences are anathema to many liberal scientists and it conflicted with the policies preferred by major science funders. A difference of political opinion also grounded in science and reason shouldn’t be that big of a deal, but for some reason it was. Major science funders, most of all the head of NIAID Dr. Anthony Fauci and the head of NIH Francis Collins, strongly believed that a better policy was to contain the virus – not mitigate its impacts – and hold off infections until vaccines arrived. The cost-benefit analysis of Fauci et al. differed from the GBD in that it prioritized only COVID mortality; costs were ignored and benefits assumed. Science, however, can’t decide which policy is better. The choice of what we ought to do is a problem as old as humanity, it is ethics and politics, religion, and morality. Thankfully, that’s why our system of government has a constitution and system of laws that provide us procedures for choosing policies even when equally good people disagree. Constitutions and procedures be damned.Drs. Fauci and Collins, both unelected and consequently not able to be unseated in an election, demanded a “devastating take-down” of the Great Barrington Declaration. They used their positions of immense scientific power to prod and poke and goad scientists who depend on Fauci and Collins for funding into action, generating a flurry of articles and media appearances calling the Great Barrington Declaration “fringe” and thereby imposing even stronger informal social control on scientists than that displayed during Ioannidis’ chapter of this saga. If you agreed with the GBD, you too were considered “fringe,” you were considered a “far-right Trump-supporting Libertarian.” That shouldn’t be a dis-qualifier in a sane scientific society, but such an accusation carries significant career costs in our politically siloed body of scientists.  Prof. Gavin Yamey MD MPH-tweets-2021-2022
After lockdowns, there were mask mandates and vaccine mandates. If you spoke up against vaccine mandates, whether your reasoning was scientific, religious, or political-philosophical, many scientists believed your speech should be labelled “disinformation.” Scientists, with the immense narrative power granted to them during this emergency, succeeded in labelling a great deal of information as “disinformation,” including scientific information such as early findings that immunity to COVID – including vaccine-induced immunity – may wane.
So some – not all – scientists did indeed fight too hard in our democratic society and their insensitive need to have everything their way risked tearing the delicate fabric of our society. They tried to force policies on people that conflicted with people’s beliefs, values, or even constitutional rights. Many people are predictably not happy about that. People spoke up and advocated for their beliefs as they are free to do in our society.
Some scientists tried to push back harder by saying that masks, lockdowns, vaccine mandates, and school closures were what The Science demanded. People, including many scientists like myself, then focused their criticism at this small band of authoritarians calling themselves The Science and interfering with our country’s representative and more inclusive policy process.
As people revolted to these Scientists’ undemocratic policies, our elected officials took note. Our democratic republic of states was a checkerboard of policies where not everyone Followed the Science, exactly as our laboratory of democracy was intended to be, but many scientists share the political belief that states’ departures from One Policy was immoral and unscientific (one and the same, in the ethical doctrine of The Science) and that the federal government should decide most things. Incidentally, the federal government is also a hub of scientific power with science-led agencies like the CDC, NIH/NIAID, and so concentrating power in the federal government would benefit scientists whereas letting states chose policies would put the decisions about public health closer to the people and their local elected representatives..
There was tension between the people, our local representatives, our federal representatives, and the Scientists. There was litigation challenging scientists’ suppression of speech, including Missouri v. Biden where plaintiffs include GBD authors were claiming Drs. Fauci and Collins infringed upon their freedom of speech by censoring these scientists and their sincerely held scientific and science-policy beliefs. There were court cases about masks on a plane that challenged the federal government’s deference of public health policy authority to unelected scientists. There were arguments aplenty, and scientists like Drs. Fauci or Hotez who felt they were lionized during the pandemic, who underwent an apotheosis to scientific authoritarianism in their pursuit of scientific saviorism, are now being bombarded by criticism from people, counties, states, elected representatives, and even scientists.
To make matters worse, one of the most consequential conflicts of interest in human history lurked beneath the surface. The virus that triggered the emergency was most likely a laboratory accident from a laboratory that received funding from these same heads of health science funding, Drs. Fauci and Collins. In fact, Peter Hotez himself subcontracted work to the Wuhan Institute of Virology. It’s within the realm of possibility the NIAID money Hotez sent to Wuhan could’ve bought the exact pipette or restriction enzymes that caused the pandemic. That’s a conflict of interest when it comes to deciding policies to mitigate the harms of this likely research-related accident.
Even without knowing the virus emerged from a lab, the mere fear they could be responsible for a global pandemic causing millions of deaths could reasonably be sufficient to cause scientists like Fauci and Hotez to exert undue influence on science and public health policy. Fears of a lab origin could explain why lab origin theories were branded as “conspiracy theories” with support from Drs. Hotez, Fauci and other health-science funders and the scientists close to them (Andersen, Holmes, Garry, etc).
Fears of a lab origin could explain why this syndicate of scientists prioritized reducing COVID mortality through extreme measures like lockdowns instead of drawing on decades of public health science by acknowledging competing risks, encouraging participation from anthropologically diverse people whose policies are being decided, and managing the more conventional all-cause mortality and morbidity instead of implementing a myopic focus on COVID.
The latter policy, incidentally, was that proposed by the GBD, none of whose authors were engaged in risky virological work in Wuhan and all of which had clear heads and sound arguments. Fears of a lab origin could plausibly lead scientists, concerned of their moral failings in possibly causing a pandemic, to desperately need a scientific saviorism success story like vaccines to balance the scales saving as many millions of lives as the millions of deaths they may have caused, leading them to label scientists’ divergent views on costs and benefits of vaccines as “disinformation.” The Wuhan COI could easily affect the observed irrational need to censor opposing views.
When we look at the pandemic history and our post-pandemic society from a more objective, less conflicted lens closer to the bodies of us innocent and diverse people Hotez labels “Anti-Science” from his siloed distance, we don’t see anything like “Anti-Science.” Instead, we see scientific authoritarianism and a predictable bipartisan anti-authoritarian response that even many scientists (including liberals like myself) support. Drs. Hotez and Fauci were authoritarians and now they are being challenged by the indomitable public that is reminding everyone who is in charge. As these authoritarians amongst us are being unseated from power, they create all manners of conspiracy theories and alternative narratives in a desperate effort to find purchase. If they can’t secure their newfound power, at least they may protect their reputations by casting their opponents as evil.
“Anti-Science” is thus not a real thing, nor is it sufficiently widely observed to warrant the dignity of being called a social construct. Anti-Science is an ego-defensive figment of Dr. Hotez’s authoritarian imagination, it is an effort to recenter The Science – the syndicate of scientists who attempted to center their own scientific paradigms and their own policy perspectives as if they were universally true and not merely political beliefs or value statements, possibly heavily conflicted ones – as deserving of power, sympathy, defense, and trust. Dr. Hotez is staring at the narrative mirrors the public uses to show him the monster he’s become, he is seeing a horrific – and true – reflection of scientists like him during the pandemic, and he is desperately trying to restore the image of himself from the current fallen general of an epistemological banana republic, back to the lionized Science and the Scientific Saviors we Followed. Hotez uses Anti-Science as an armor and an excuse to bypass a critical self-examination of the possible insensitivity and undemocratic behavior of he and his scientific savior colleagues during the pandemic.
The best way to assess whether a thing is objective or subjective is to ask different people if they see the same thing. That’s science. Of course, for things that hurt people like micro aggressions and the likes, it may help to ask the victims if it exists as they should experience the concentrated effects of the thing. I am a scientist, I was involved in both science and public policy during COVID, and yet I don’t see any horror of “Anti-Science” along my path in this narrative house of horrors.
Sure, I’ve seen disagreements in the public melee. I remember the history of disinformation on climate science, tobacco, and even Russian disinformation on all things, but that is not the thing Hotez describes and there isn’t generality other than institutions protecting their self-interests not because they are “Anti” anything but because they are “Pro” self and sometimes science reveals information that hurts a business’s bottom line. I’ve also seen companies act the same way when competitors enter the market, so past conflicts have nothing to do with science specifically. I’ve even been attacked, and even attacked for my science, but mostly I’ve been attacked by other scientists (including Hotez) who disliked the political implications of my findings. The Scientists who attacked me all form a relatively small, insular network of people closely connected with NIAID, NIH, or EcoHealth Alliance. While I was a researcher in the same wildlife virology community as EcoHealth Alliance, I didn’t conduct gain-of-function research, I didn’t subcontract work to the Wuhan Institute of Virology, and I have maintained objectivity by critically evaluating the facts of the matter even where they inconveniently point to scientists’ mismanagement of risks. I’ve found flaws in Science papers and used my expertise to uncover evidence consistent with SARS-CoV-2 being a research product of EcoHealth Alliance’s pre-COVID research proposals.
I critically examined early case data, found evidence of large pools of unascertained cases consistent with a lower-severity pandemic and was told that my science risked “upsetting public health policy.” I argued otherwise, helped in part by my brilliant wife who has a PhD in public health policy. I argued that the only way sincere science and rigorous analyses could “upset public health policy” would be if public health policy were unscientific, if scientists were usurping the public’s seats in the policy process, centering Scientists, their belief systems, their value systems, and their institutions at the expense of decentering a larger, more diverse public. I found evidence that corroborated the Great Barrington Declaration’s cost-benefit analysis, and I shared that evidence privately with policymakers without grabbing the reigns and forcing them to choose any one policy.
As a scientist who maintained independence, who presented evidence without invading the deliberative jury or the policy process, I see scientists who became intolerant, petulant authoritarians; I don’t see “Anti-Science” as anything other than a reflection of Hotez grappling with the legitimate criticisms of his and his colleagues’ improper authoritarian scientific conduct before, during, and after the pandemic.
Far from being “anti-scientific,” the anti-authoritarianism unseating Hotez as one of the hallmarks of a true scientist and it is a hallmark of the people our republic. You don’t have to be an expert historian or anthropologist to recall that Americans went to war with the British because my ancestors despised authoritarians ruling without representation.
Throughout the pandemic, many members of the public have been better scientists than many prominent scientists. Members of the public and independent scientists have resisted convenient explanations when the data did not support them, such as the claim that lockdowns are indisputably wise policies when the public knew that lockdowns carried costs that were not being considered by scientists like Hotez on MSNBC.
Members of the public and independent scientists have rightfully questioned the efficacy of masks, and only years later are their hunches about the low efficacy or possible inefficacy of masks as a public health policy becoming known by scientists.
Members of the public and independent scientists questioned the safety and efficacy of vaccines, especially at reducing the risk of infection in the long term, and slowly, only after being labelled as “disinformation,” we are obtaining evidence of myocarditis, vaccine evasion in Provincetown, and more. Our citizenry has proven brilliant and remarkably agile, and predictably anti-authoritarian.
Hotez calls anyone – even scientists – assessing possible costs and estimating the true benefits of vaccines as “anti-vax.” It’s not “anti-vaccine” to err on the side of caution, to help doctors maintain their Hippocratic oath by ensuring benefits of a treatment or vaccine exceed the risks on a case-by-case basis (in science, we call this “individualized medicine”).
On the contrary, supporting systems that shake down and test hypotheses of vaccine safety and efficacy is one of the most pro-vaccine things we can do as it will inspire trust in vaccines that survive the gauntlet of scientific cross-examination. It is both pro-vax and pro-science to question the safety and efficacy of treatments, even those that have passed clinical trials, because that process of shaking down the answers gives us more confidence in the treatments we use and the science we’ve settled on. How many treatments have passed clinical trials only to be later discovered to have intolerable side effects? Would Hotez prefer “science” not uncover such later-discoverable complications?
Similarly, it is not “Anti-Science” to question the policies recommended by scientists or to investigate the possibility that scientists caused a pandemic. What Hotez calls “Anti-Science” is the core of science itself: an independence of mind, a diversity of perspectives, and an anti-authoritarian proclivity that conflicts with the interests of authoritarians masquerading as scientists. It is this independence and anti-authoritarianism that inspires confidence in science as well as democratic society, not the toxic ramblings of a scientific authoritarian as he’s unseated from power. Republished from the author’s Substack Alex Washburne is a mathematical biologist and the founder and chief scientist at Selva Analytics. He studies competition in ecological, epidemiological, and economic systems research, with research on covid epidemiology, the economic impacts of pandemic policy, and stock market response to epidemiological news. |
|
Malice Aforethought on the COVID-19 Pandemic: “This is a global coup d’etat and intentional mass murder.” Dr. Mike YeadonBy Dr. Mike Yeadon
*** A message written to a trusted campaigning friend, who is struggling to accept that what is happening is intentional. It is indeed a big step to move from justifiable criticism of presumed incompetent politicians and industrialists to putting the pieces together in such a way that they can point only to intentionality. See what you think. * Dear X, I find that attempting to put all the information together in such a way as to allow for the whole even to be benign or at least not wholly malevolent is impossible.
That’s because, as you’ve no doubt heard me say, I believe it is malevolent! I too struggled early on, arguing “surely they must have known this!?” Etc. Once I allowed for the possibility that all the bad things were intentional, I find all the rest falls into place. Obviously that alone doesn’t prove that it was intentional.
Some early clues to intentionality are the coordinated responses of scores of governments to the alleged pandemic: lockdowns, masking, mass testing of the well, the misapplication of PCR-based techniques to bulk testing of clinical samples, selective business & school closures, border restrictions etc.
Not a single country had any of this as a core part of their own pandemic preparedness plan. Even the WHO’s scientific evaluation of NPIs concluded none of them worked & the only changes worth a dime were asking those with symptoms to remain at home until recovered & to increase the frequency of hand washing (because the route of transmission wouldn’t initially be known for sure).
I argued at the time that the only way all the countries could have adopted all these useless yet damaging & costly NPIs is if there was supranational coordination.
Whether that from WHO, WEF, etc., I don’t know. But illegitimate in any case. We now know that they knew that imposing these restrictions would save nobody, yet the negative consequences would be devastating, even lethal for some, who would no longer have access to the medical care they needed. Additionally, the use of furlough was obviously going to be enormously damaging to sovereigns who were already borrowed to the hilt.
I note the widespread adoption of an American term, furlough, into public discourse. In U.K. we never previously used the term. Nobody remarked on its arrival, which telegraphed the leading role played by Americans.
Then we have the imposition of radically altered medical protocols. Because of my long exposure to matters respiratory, I knew immediately they began panicking about needed 30,000 mechanical ventilators that something truly demonic was at hand. It’s never appropriate, in a patient with an unobstructed airway & an intact chest wall to sedate, intubate and ventilate them. Mechanical ventilation is certainly a marvellous, life-saving thing, but it comes with serious risks to the frail patient, in the form of ventilator acquired pneumonia, lung injury from use of pressure to inflate the lungs and more. The appropriate treatment would be an oxygen mask, single, low dose benzo, a cup of tea and a biscuit and a caring hand upon an arm.
In the USA as well many, once in this vulnerable state, were given remdesivir & not given total, intravenous nutrition. In most cases it was just a matter of time before they died.
In care homes, there was indiscriminate use of inappropriately high doses of midazolam and morphine. Not only high doses but repeatedly given to their elderly charges. They’d been told to do it by the highest medical authorities in the land and so few questioned it.
My PhD by coincidence was in this area, the effect of opiates on respiratory function. The discovery of multiple opiate receptors raised the possibility that it might be possible to invent receptor selective ligands that would relieve pain with reduced respiratory depression. Unfortunately, both are mediated primarily by mu opiate receptors, both centrally and in the periphery.
The combination of opiate agonists and benzodiazepines is contraindicated in patients unless close monitoring (for signs of respiratory depression) was in place.
It isn’t & cannot be in a care home. They too were murdered in large numbers. Finally, in the community, the family doctors were cautioned not to prescribe antibiotics in cases of covid “because antibiotics cannot treat viral illnesses”. It’s well known that what is usually termed secondary bacterial infection is generally what actually leads to death in this situation. However, the records show that prescriptions for antibiotics for suspected bacterial infection of the lungs fell by 50% & large numbers of people died avoidable deaths (and rather horrible deaths, too).
It’s not possible to regard all of this evidence without concluding that malice aforethought was at work here. It’s literally diabolical, what they did.
How it was done with so little pushback still confuses me. I do know that from the late-1990s right through late-2019, there was a sequence of tabletop simulations of global pandemic scenarios & bioterrorism scenarios, which allowed the perpetrators to hone their craft in the responses & control measures imposed. I believe some of these were translated onto the ground, giving emergency response team a chance to form & to rehearse what most of them thought were appropriate, given the fictional set up, though this is speculative.
Then we come to the “vaccines”. Given a career in pharma and biotech, I knew that it was impossible to create a vaccine in under 5-6 years if they were going to demonstrate clinical safety and hone manufacturing to yield the customarily high quality manufacturing necessary to produce tightly defined final drug product. If the latter if not done, it’s pointless doing the former, because what would otherwise be injected wouldn’t be what had been used in the clinical trials.
In other words, if there was a need for a new vaccine, you would never even contemplate running such a program, because no pandemic in history lasts a fraction of the minimum time necessary to create a safe and effective new vaccine.
Yet they went ahead. This too is malevolent, let alone the extraordinary lying, censorship & smearing of dissenters. Given my entire career used “rational drug design” principles to design and test molecules, I was able to put myself in the shoes of the designers of the jabs.
There are several, completely obvious safety issues built into these products. One is the axiomatic induction of “autoimmune” responses, regardless of which antigen was selected. The next was choice of antigen, where no one would pick spike protein, because it was highly likely to be directly toxic, it’s subject to the most rapid mutation (so a vaccine might lose efficacy) & also it’s the least different from human proteins (and so might trigger bystander attacks on even somewhat similar self proteins).
Yet all four leading players chose this antigen. What a coincidence! I’d have called up my peers in the other companies to endure we didn’t do that. That’s because it would be highly undesirable to have common risks to all programs.
On formulation, the mRNA-based products both selected LNPs to encapsulate their message. Yet there was industry knowledge that these not only travel all over the body including into the brain but that they accumulate in the ovaries.
Yet, knowing this, the companies & regulators went ahead and then others compounded the toxicity risk by recommending these injections in pregnant women and children.
I was still slow to piece together all this evidence of carefully thought out harms. But eventually I got there and have been speaking in what many regard as extreme terms ever since.
I’m afraid there’s no hiding from the reality that this is a global coup d’etat and intentional mass murder. Worse, we see the encroachment of surveillance technology and legal powers to introduce digital ID & CBDC as well as to eliminate cash.
It’s not difficult to come up with scenarios where presentation of digital ID will become mandatory. * Note to readers: Please click the share button above. Follow us on Instagram and Twitter and subscribe to our Telegram Channel. Feel free to repost and share widely Global Research articles. Dr. Michael Yeadon, PhD, was Formerly Vice President & Chief Scientific Officer Allergy & Respiratory at Pfizer Global R&D. He holds Joint Honours in Biochemistry and Toxicology and a PhD in Respiratory Pharmacology. He is an Independent Consultant and Co-founder & CEO of Ziarco Pharma Ltd.
|
|
The Great Demoralization26September2023 Updated: 26September2023 https://www.theepochtimes.com/opinion/the-great-demoralization-5498920
Commentary On March 6, 2020, the mayor of Austin, Texas, canceled the biggest tech and arts trade show in the world, South-by-Southwest, only a week before hundreds of thousands were to gather in the city.
In an instant, with the stroke of a pen, it was all gone: hotel reservations, flight plans, performances, exhibitors, and all the hopes and dreams of thousands of merchants in the town. Economic impact: a loss $335 million in revenue at least. And that was just to the city alone, to say nothing of the broader impact.
It was the beginning of U.S. lockdowns. It wasn’t entirely clear at the time—my own sense was that this was a calamity that would lead to decades of successful lawsuits against the Austin mayor—but it turned out that Austin was the test case and template for the entire nation and then the world.
The reason was of course COVID but the pathogen wasn’t even there. The idea was to keep it out of the city, an incredible and sudden fallback to a medieval practice that has nothing to do with modern public health understanding of how a respiratory virus should be handled.
“In six months,” I wrote at the time, “if we are in a recession, unemployment is up, financial markets are wrecked, and people are locked in their homes, we’ll wonder why the heck governments chose disease ‘containment’ over disease mitigation. Then the conspiracy theorists get to work.”
I was right about the conspiracy theorists but I had not anticipated that they would turn out to be right about nearly everything. We were being groomed for extended national and global lockdowns.
At this point in the trajectory, we already knew the gradient of risk. It was not medically significant for healthy working-age adults (which still to this day the CDCs does not admit). So the shutdown likely protected very few if anyone.
The extraordinary edict—worthy of a tin-pot dictator of a dark age—completely overrode the wishes of millions, all on the decision of one man, whose name is Steven Adler.
“Was the consideration between maintaining that money, effectively rolling the dice, and doing what you did?” asked Texas Monthly of the mayor.
His answer: “No.” Clarifying: “We made a decision based on what was in the best health interest for the city. And that is not an easy choice.”
After the shocking cancellation, which overrode property rights and free will, the mayor urged all residents to go out and eat at restaurants and gather and spend money to support the local economy. In this later interview, he explained that he had no problem keeping the city open. He just didn’t want people from hither and yon—the dirty people, so to speak—to bring a virus with them.
He was here playing the role of Prince Prospero in Edgar Allan Poe’s “The Masque of the Red Death.” He was turning the capital city of Texas into a castle in which the elite could hide from the virus, an action that also became a foreshadowing of what was to come: the division of the entire country into clean and dirty populations.
The mayor further added a strange comment: “I think the spread of the disease here is inevitable. I don’t think that closing down South Bay was intended to stop the disease from getting here because it is coming. The assessment of our public health professionals was that we were risking it coming here more quickly, or in a greater way with a greater impact. And the longer we could put that off, the better this city is.”
And there we have the “flatten the curve” thinking at work. Kick the can down the road. Postpone. Delay herd immunity as long as possible. Yes, everyone will get the bug but it is always better that it happens later rather than sooner. But why? We were never told. Flatten the curve was really just prolong the pain, keep our overlords in charge as long as possible, put normal life on hold, and stay safe as long as you can.
Prolonging the pain might also have served another surreptitious agenda: let the working classes—the dirty people—get the bug and bear the burden of herd immunity so that the elites can stay clean and hopefully it will die out before it gets to the highest echelons. There was indeed a hierarchy of infection.
In all these months, no one ever explained to the American public why prolonging the period of non-exposure was always better than meeting the virus sooner, gaining immunity, and getting over it. The hospitals around the country were not strained. Indeed, with the inexplicable shutdown of medical services for diagnostics and elective surgeries, hospitals in Texas were empty for months. Health care spending collapsed.
This was the onset of the great demoralization. The message was: your property is not your own. Your events are not yours. Your decisions are subject to our will. We know better than you. You cannot take risks with your own free will. Our judgment is always better than yours. We will override anything about your bodily autonomy and choices that are inconsistent with our perceptions of the common good. There is no restraint on us and every restraint on you.
This messaging and this practice is inconsistent with a flourishing human life, which requires the freedom of choice above all else. It also requires the security of property and contracts. It presumes that if we make plans, those plans cannot be arbitrarily canceled by force by a power outside of our control. Those are bare minimum presumptions of a civilized society. Anything else leads to barbarism and that is exactly where the Austin decision took us.
We still don’t know precisely who was involved in this rash judgment or on what basis they made it. There was a growing sense in the country at the time that something was going to happen. There had been sporadic use of lockdown powers in the past. Think of the closure of Boston after the bombing in 2013. A year later, the state of Connecticut quarantined two travelers who might have been exposed to Ebola in Africa. These were the precedents.
“The coronavirus is driving Americans into unexplored territory, in this case understanding and accepting the loss of freedom associated with a quarantine,” wrote the New York Times on March 19, 2020, three days after the Trump press conference that announced two weeks to flatten the curve.
The experience on a nationwide basis fundamentally undermined the civil liberties and rights that Americans had long taken for granted. It was a shock to everyone but to young people still in school, it was utter trauma and a moment of mental reprogramming. They learned all the wrong lessons: they are not in charge of their lives; someone else is. The only way to be is to figure out the system and play along.
We now see epic learning loss, psychological shock, population-wide obesity and substance abuse, a fall in investor confidence, a shrinkage of savings reflecting less interest in the future, and a dramatic decline in public participation in what used to be normal life events: church, theater, museums, libraries, fairs, symphonies, ballets, theme parks, and so on. Attendance in general is down by half and this is starving these venues of money. Most of the big institutions in large cities like New York, such as Broadway and the Met, are on life support. The symphony halls have a third empty seats despite lowering prices.
It seems remarkable that this three-and-a-half year-long war against basic liberty for nearly everyone has come to this. And yet it should not be a surprise. All ideology aside, you simply cannot maintain much less cultivate a civilized life when governments, in combination with the commanding heights of media and large corporations, treat their citizens like lab rats in a science experiment. You only end in sucking away the essence and vibrancy of the human spirit, as well as the will to build a good life.
In the name of public health, they sapped the will to health. And if you object, they shut you up. This is still going on daily.
The ruling class that did this to the country has yet to speak honestly about what transpired. It was their actions that created the current cultural, economic, and social crisis. Their experiment left the country and our lives in shambles. We’ve yet to hear apologies or even basic honesty about any of it. Instead, all we get is more misleading propaganda about how we need yet another shot that doesn’t work.
History provides many cases of a beaten down, demoralized, and increasingly poor and censored majority population being ruled over by an imperious, inhumane, sadistic, privileged, and yet tiny ruling class. We just never believed we would become one of those cases. The truth of this is so grim and glaring, and the likely explanation of what happened so shocking, that the entire subject is regarded as something of a taboo in public life.
There will be no fixing this, no crawling out from under the rubble, until we get something from our rulers other than public preening about a job well done, in ads sponsored by Pfizer and Moderna. From the Brownstone Institute Views expressed in this article are opinions of the author and do not necessarily reflect the views of The Epoch Times.
Jeffrey A. Tucker |
|
Steve Kirsch’s newsletterUS Nursing home data shows clearly that the COVID vaccines were a disaster for the elderly; they increased the risk of dying from COVIDI’m going to drill into more detail on this analysis of the CDC “gold standard” database which shows that the vaccines were a huge failure. There is no way to put a positive spin on this.Steve Kirsch 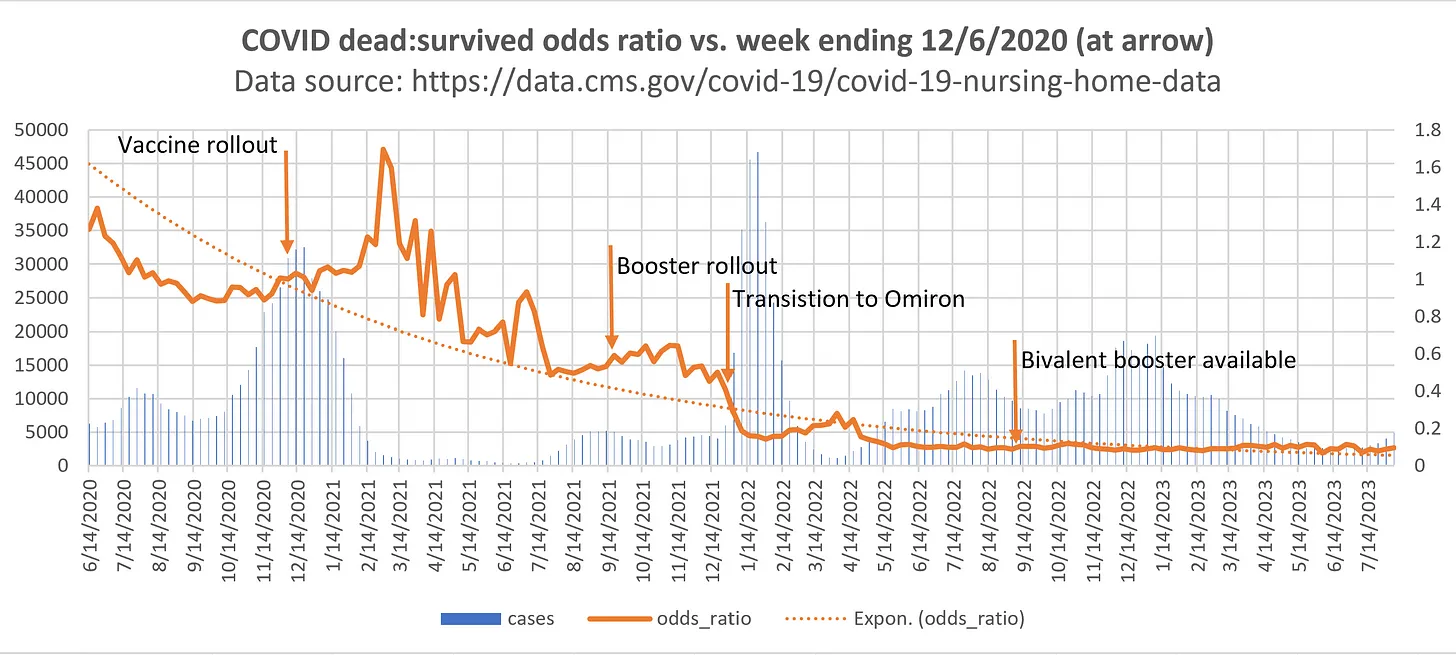 COVID dead: survived odds ratio vs. week ending 6December2020 (at arrow)
Executive summaryThe US Nursing Home data is the “gold-standard“ record level data for what happened in nursing homes after the COVID vaccine rolled out.
The signal from this data is clear and unambiguous: both the primary series and booster COVID vaccines increased the risk of death from COVID. The bivalent vaccines did absolutely nothing for the elderly (at least it didn’t make things worse, but it didn’t make things better).
The two things that reduced the infection fatality rate (IFR) were:
We can see both effects very clearly in the data shown in Figure 1 above. This is why the CDC isn’t touting this database as proof that the vaccines work. Neither is anyone on the pro-vax side of the narrative despite the fact that this data has been in public view for 2 years now.
So since nobody from their side wanted to analyze the data, I thought it would be a good idea if someone from our side took a look.
The reason why they never wrote about this to prove their case is that it shows the opposite. The so-called “misinformation spreaders” have been right all along: the vaccine clearly significantly increased the risk of an elderly person getting COVID for around 4 months. This is a huge problem because this was the time when the vaccine was supposed to be most effective (since we now know from FOIA requests that the FDA knew that the vaccine protection waned after 4 months).
Health officials claimed the vaccine could reduce risk of death by 10x. It’s right here in this tweet from an Australian government health authority NSW Health on August 17, 2021: 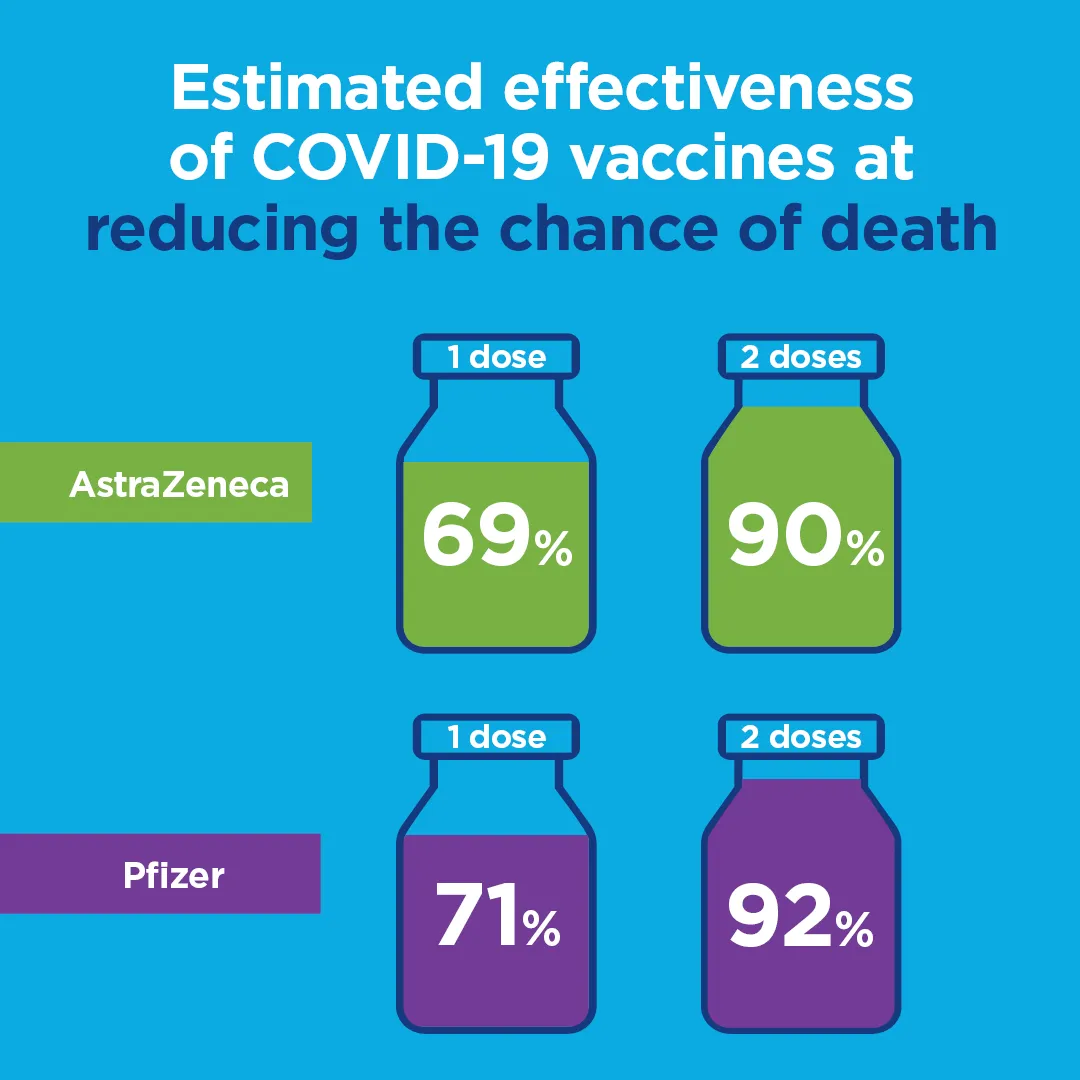 Estimated effectiveness of COVID-19 vaccines The data they never told us about (the US Nursing Home data) shows a completely different story: it did the opposite and increased the risk of death by as much as 1.6 times higher odds of dying.
The attempts to attack my analysis, to date, are addressed here. They are weak hand-waving arguments with no evidentiary support. At no time did anyone ever justify their arguments with any numbers derived from the data. None of the attackers will publish their “correct” analysis of this data or their investigations showing anomalies.
The fact is that this is “gold standard” data. It doesn’t get any “closer to the source” than this. There were over 2M records to analyze from over 15,000 elderly care facilities in the US. These are large numbers and the effect size was huge.
The Fisher exact p-value for the 1.7 OR peak on 2/28/21 is 2.6e-109 and the Z-score for the odds ratio is 23.53. In other words, this difference didn’t happen because I cherry picked a result or it happened by chance. It was caused by something. If it wasn’t the vaccine, what caused this statistically significant difference in the rate of death from the virus (it was the same variant as before the vaccines rolled out).
Equally important is that Apple Valley Village had a 0% death rate from COVID prior to the vaccine rollout: 26 infections and not a single death. Just 3 weeks after the week of the shots, they had 90 COVID infections which resulted in 28 deaths from COVID. My hypothesis can easily explain that. Theirs cannot. So you can throw all the FUD you want at the Nursing Home data, but the bottom line is that this one anecdote is very powerful because it is verifiable in the database and with employees, but it cannot be explained how the death rate in this nursing home suddenly got at least 9X worse after the shots rolled out that should have made the death rate 10X better. That is a 70X swing. This is why Professor Morris simply ignores this because he cannot explain it. In science, you can’t ignore data you don’t like. You have to be able to explain it or admit you cannot. Morris does neither.
Don’t you find it strange that this data has been publicly available for two years now and not a single pro-vaccine advocate has analyzed it and is touting it as “proof” the vaccines work? At this point, the medical community has a choice: embrace the data and admit you were wrong or try to fight it. History will not look kindly on attempts to dismiss this data. The first rule of holes: if you find yourself in a hole, stop digging. They are in a big hole. What will they do now? Data availabilityCode: You can find everything in my github repo here. Nursing home data: You can download the data from my repo or directly from CMS. Now, where are the repos of others who have analyzed this data? They do not exist as far as I know. How is that possible? Why can’t we see their work? Key documentsPreparing for COVID-19 in Nursing Homes shows that the policy in effect on November 20, 2020 and beyond was to test all new admissions into nursing homes and anyone who is symptomatic. I verified this practice was followed by talking to people who work in the nursing care homes. So the claim that people who transferred into nursing homes didn’t get tested is without evidentiary support.
Boosters were rolled out starting on September 20, 2021. See: Nursing homes charging ahead to administer COVID-19 vaccine booster shots The bivalent booster was first available in the United States nearly one year later on September 1, 2022. Nursing homes site of 40% of US COVID-19 deaths shows that nursing homes are ground zero for the vaccine. If it doesn’t work there, it is a failure. What I foundEverything is summarized in the Executive Summary at the start. The key point is that, in aggregate, when compared to pre-vax infection fatality rates, the odds of death climbed for months after the vaccines were delivered when they were “supposed to” have fallen like a rock. In particular the odds of death ( deaths from covid:survivors from COVID) increased post-vaccine. So did the absolute risk reduction; it went south which means the vaccines increased your risk of death. In short, the vaccine made things worse. The reference point chosen (the week prior to vaccine rollout) is immaterial; the slopes all went the wrong way. There is no doubt about this. This is a huge failure of the vaccine.
In addition, the virus has mutated to Omicron which isn’t killing anyone. Boosters are silly. They should be ashamed of themselves for pushing this when there clearly isn’t a problem. 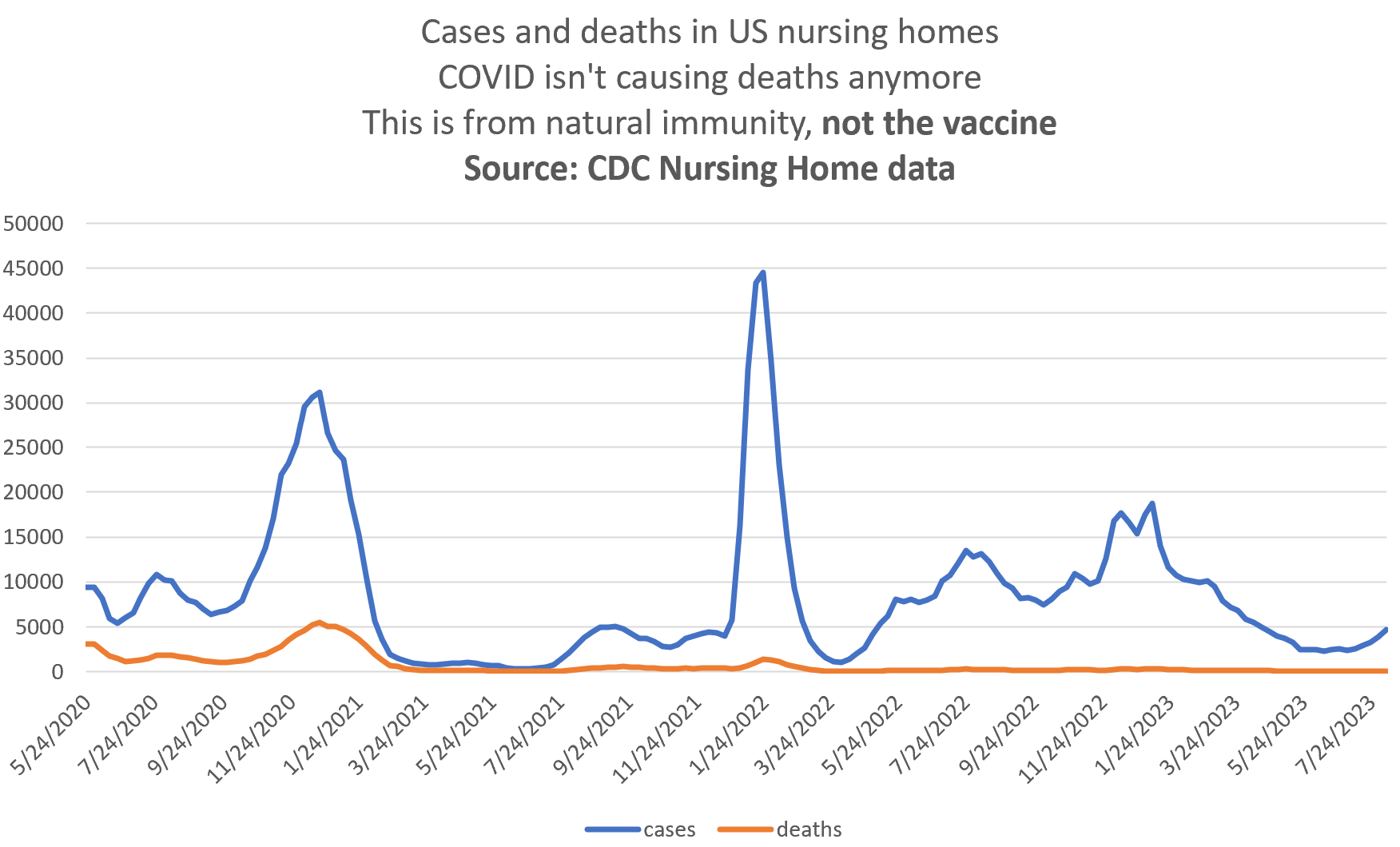 Cases and deaths in US nursing homes
Could this analysis be wrong? Could the vaccine have saved lives?No. Anecdotes like Apple Valley Village (mentioned above) are unexplainable. The Pfizer Phase 3 clinical trial had more all-cause deaths in the treatment group than the placebo group, but the numbers were too small to be statistically significant. So the trials provide no visibility into the death “benefit.”
There are many others who have pointed out issues with the vaccines including this amazing video by John Beaudoin and the 1,200 articles I’ve written on my Substack. Why did this happen?Is there a biological basis for how the vaccine can make things worse? Yes! The vaccine damages your immune system. See this article by Igor Chudov for a clinical trial done on kids with healthy immune systems. Previous articlesSee:
The attempts to discredit the data and/or analysisHere are the attempts to discredit my analysis of this data. At no point do any of these people point to the “correct” analysis showing that the data shows the vaccines reduced the death rate. Nor do any of the attacks actually have any numbers. They are all hand-waving attacks with no evidentiary support. The attack is in bold, the responses follow.
If you want to read Professor Morris’s critique in his own words, you can find it here. Here are the quick answers to each item.
I found his arguments lacking in any data or numbers to back them up. And he completely failed to explain AVV; he wouldn’t even attempt it.
I also invited him to submit to me his anecdote of a success case where the IFR in the nursing home dropped by 9X or more. I’d love to see it. After all, there should be hundreds of such homes. Can he name one? The NSW government promised the OR would drop like a lead balloonAs noted above, the NSW Health authority claimed that risk of death drops by 10X. I’d love to see how the OR of death goes to .1 after the vaccine. Where is the data? Where is their analysis of the CMS Medicare data?This is gold standard data. They should be touting it. It’s been up for 2 years. Nothing. Not a peep. Nobody touched it. It’s basically a third rail for the narrative.
40% of the COVID deaths were in US nursing homes, so this is the #1 demographic to examine. The data was there. Why did they ignore it? If there is a mortality benefit, where is the benefit curve post-vax and why is this kept hidden?Where is their curve of the odds ratio of death from COVID post vaccine? I haven’t seen it anywhere. I asked Professor Morris for the correct IFR since he claims mine is wrong. He could not provide it. If he doesn’t know the correct numbers, how can he know my numbers are wrong? For more infoSee my previous article where it talks about the only paper published referencing this data See also my Twitter post:
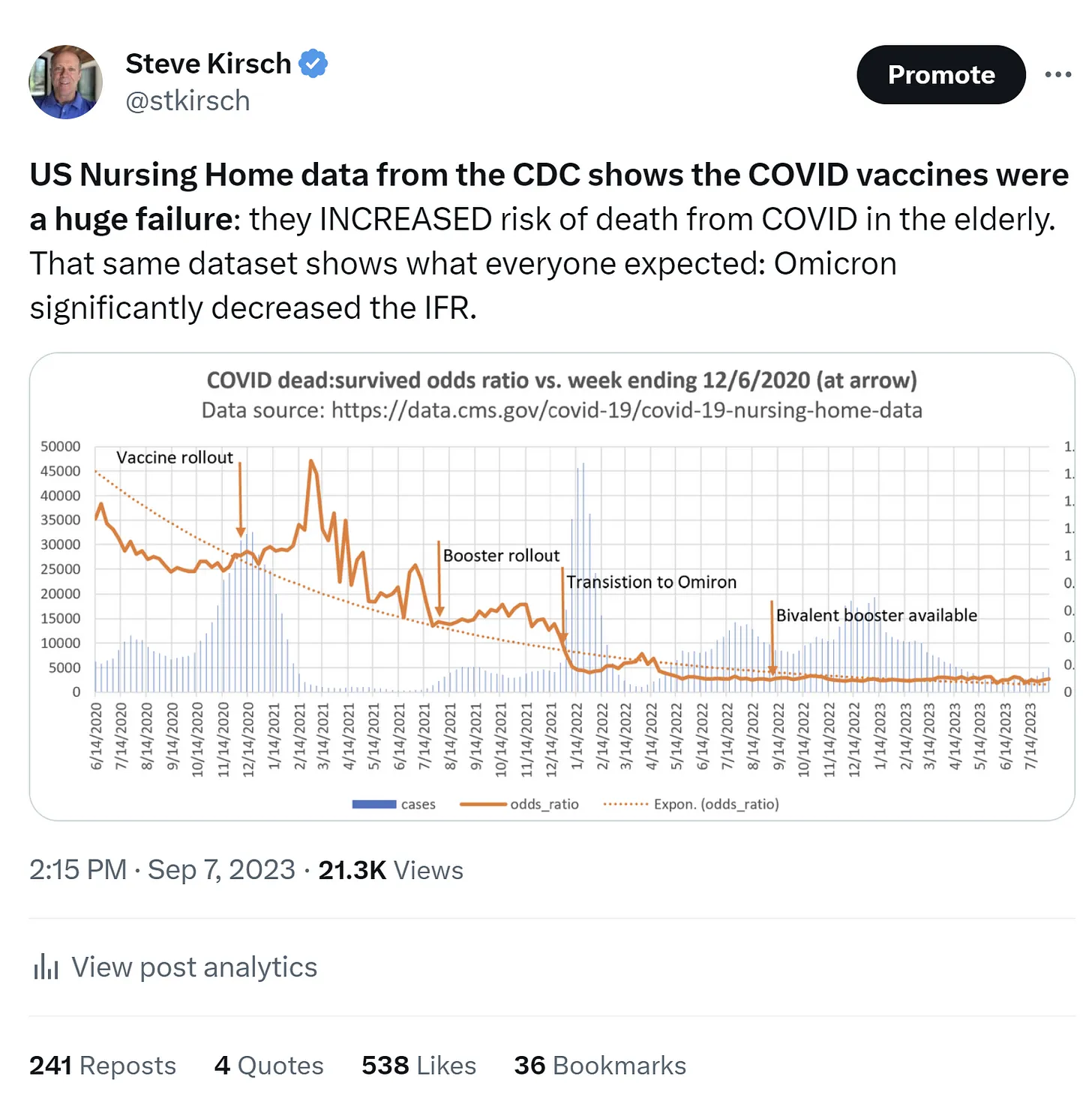 Steve Kirsch-tweet-7September2023-US Nursing Home data from the CDC shows the COVID vaccines were a huge failure SummaryThe vaccines made things worse for the very population that it was supposed to help.
That’s why nobody ever published a favorable analysis of the US Nursing Home Data even though it has been out for 2 years.
The vaccines shouldn’t be used by anyone, especially those with a compromised immune system. It damages your immune system. People with a damaged immune system will be left with an even more damaged immune system.
When will the medical community acknowledge they made a huge mistake?
|
|
Some COVID Vaccines Produce ‘Unintended Immune Response’ in Recipients: StudyThe COVID vaccines were fundamentally faulty, revealed researchers, as they reworked the synthetic mRNAs to prevent further harmful responses.By Naveen Athrappully
Researchers in a landmark new study have discovered a sequence within the Pfizer mRNA vaccine that produces an “unintended immune response” in the body, which experts are calling a massive “developmental and regulatory failure.”
Synthetic Messenger Ribonucleic Acid (mRNA), such as that used in Moderna and Pfizer vaccines, enables the body to create a specific spike protein mimicking SARS-CoV-2. The body reacts to the foreign protein and generates protective immunity, which theoretically neutralizes the real virus when it enters the body.
“Researchers from the Medical Research Council (MRC) Toxicology Unit have discovered that the cellular machinery that ‘reads’ mRNAs ‘slips’ when confronted with repeats of a chemical modification commonly found in mRNA therapeutics. In addition to the target protein, these slips lead to the production of ‘off-target’ proteins triggering an unintended immune response,” said a press release for the study published in Nature on Dec. 6.
The MRC team redesigned the mRNA vaccine to prevent further harmful immune responses from the spike proteins. “The researchers identified that bases with a chemical modification called N1-methylpseudouridine—which are currently contained in mRNA therapies—are responsible for the ‘slips’ along the mRNA sequence.”
When the MRC team collaborated with researchers from the Universities of Kent, Oxford, and Liverpool, they found an unintended immune response occurred in one-third of the 21 patients in the study who were inoculated with the Pfizer mRNA vaccine. Re-Engineering mRNA
The team reengineered the error-prone genetic sequences in the synthetic mRNA to avoid these unintended and “off-target” effects.
“We can remove the error-prone code from the mRNA in vaccines so the body will make the proteins we want for an immune response without inadvertently making other proteins as well. The safety concern for future mRNA medicines is that misdirected immunity has huge potential to be harmful, so off-target immune responses should always be avoided,” said Dr. James Thaventhiran from the MRC team, who is also a practicing clinician at Addenbrooke’s hospital.
Biochemist Professor and MRC team member Anne Willis said that the redesigning work presents “both a concern and a solution for this new type of medicine.”
Ribosomes in cells produce proteins from natural and synthetic mRNAs, and a precise positioning of the ribosome on the mRNA is needed to make the right proteins. The ribosome ‘reads’ the mRNA sequence three bases at a time, and any tiny deviation that happens here “massively distorts the code and the resulting protein,” said the Cambridge press release.
When the ribosome misreads the mRNA and ends up with unintended amino acids, the mutation is known as a frameshift. “When the ribosome is confronted with a string of these modified bases called N1-methylpseudouridine in the mRNA, it slips around 10% of the time, causing the mRNA to be misread and unintended proteins to be produced—enough to trigger an immune response. Removing these runs of N1-methylpseudouridine from the mRNAs prevents ‘off-target’ protein production.”
This research was funded by the Medical Research Council and the Wellcome LEAP R3 program, and supported by the NIHR Cambridge BRC. As for competing interests, two of the authors in the study are inventors on a pending patent application (2305297.0) related to mRNA technology. Fundamental FailureAlthough the MRC team insisted that the unintended immune responses were found to have no ill effects, expert responses to the study claimed the safety concern revealed a more fundamental failure of the scientific and regulatory communities in approving the COVID mRNA vaccines.
“The formation of these off-target proteins is not disclosed in the package insert for COMIRNATY,” said a commentary on the study published in ResearchGate. “The finding that unintended proteins may be produced as a result of vaccination is sufficient cause for regulators to conduct full risk assessments of past or future harms that may have ensued.”
Authors said that according to WHO guidelines for mRNA vaccines, “manufacturers should provide details of ‘unexpected ORFs’ (Open Reading Frames),” referring to cellular modification on a DNA level.
“Given that this study was conducted under the auspices of the United Kingdom Government, we must assume UK regulators, manufacturers, and international regulatory agencies, including FDA, were apprised of the data many months ago.
“We await their account of what steps they have taken to investigate why the formation of off-target proteins was not discovered sooner, what toxic effects they may have caused, and what steps they are taken to prevent harm in the future and to inform the public of these findings.”
The Epoch Times reached out to Pfizer, Moderna, the FDA, and the CDC for comment. Social Responses
In a Dec. 6 post on X, Dr. Jonathan Engler said: “This is devastating. A design flaw in the mRNA injections results in them making random proteins which will be massively pro-inflammatory. Because the product is distributed throughout the body, this happens everywhere. This likely explains the huge variety of immune disorders reported in association with these products.”
Supporters of the study claimed that critics were making an issue unnecessarily. “Frameshifts are uncommon but naturally occurring events in, for example, viral infections,” said Edward Nirenberg, a medical publisher. “These give rise to protein products that can also be targeted by the immune system.”
“Coronaviruses have evolved to require frameshifting as part of their replication cycle to make their proteins.”
Immunologist Marc Veldhoen said in an X Post: “Some well-known anti-vaxers are making claims that the ribosome slip/frameshift causes a stop codon to be missed and an own mitochondrial protein to be made, risking autoimmunity. It´s important to know that the mRNA in COVID-19 vaccines do not contain other protein codes.”
Emergency Physician Kashif Pirzada MD said in an X post: “This is a big deal. Novavax produces much milder reactions in people compared to the mRNA shots, and also presents a more conventional protein-based vaccine option in our polarized information environment. I usually get floored by the mRNA shots, not so with Novavax.”
Novavax is “probably” the safest COVID-19 vaccine compared to other brands, according to cardiologist Dr. Peter McCullough, who added that he still would not recommend the shot due to high cardiac risks posed by COVID vaccines.
The three major classes of COVID-19 vaccines are mRNA, vector, and protein subunit vaccines. The Pfizer and Moderna COVID-19 vaccines use mRNA technology, while AstraZeneca and Janssen come under the vector category. Novavax is a protein subunit vaccine.
There are multiple studies pointing to people suffering from adverse events after being vaccinated.
An October study suggested that COVID-19 vaccines could trigger rheumatic immune-mediated inflammatory diseases that involve inflammation manifesting in the joints, tendons, bones, and muscles due to an unknown cause. This includes conditions like arthritis, vasculitis, lupus, and adult-onset Still’s disease.
Research has shown that COVID-19 mRNA vaccines can reduce a beneficial gut bacteria called Bifidobacteria, the presence of which is associated with higher immunity against pathogens and cancer.
In a recent interview with the “American Thought Leaders” program, clinical pathologist Dr. Ryan Cole said that DNA contamination in some of the mRNA vaccines could be linked to a rising incidence of cancers, micro-clotting, and autoimmune diseases.
Naveen Athrappully
|
|
Study Finds Signs of Heart Injury in Vaccinated People Without Chest PainThe study results ‘suggest that mild asymptomatic myocardial inflammation could be more common than we ever expected,’ one doctor said.27September2023 Updated: 28September2023 https://www.theepochtimes.com/health/study-finds-signs-of-heart-injury-in-asymptomatic-vaccinated-people-5498717 People who received a COVID-19 vaccine had higher levels of a glucose analogue than unvaccinated people, suggesting heart inflammation, according to a new study.
Researchers in Japan compared 700 vaccinated people with 303 unvaccinated people. None experienced cardiac symptoms. Researchers analyzed results from positron emission tomography and computerized tomography (PET/CT) scans that analyzed the uptake of fluorodeoxyglucose F18 (FDG), a glucose analogue and marker of inflammation, in the body.
Researchers found that people vaccinated with a Moderna or Pfizer vaccine had higher levels of FDG in the heart, liver, and spleen than unvaccinated people.
The higher levels of heart FDG remained when stratifying the patients by various factors, such as age, except for people who were tested more than 180 days after vaccination.
The higher FDG levels represent heart inflammation, Dr. Takehiro Nakahara of the Keio University School of Medicine’s Department of Radiology and co-authors wrote. The levels could just indicate minor inflammation, they said, pointing to a cardiac MRI study that found that post-vaccination heart problems were less severe than those experienced after COVID-19.
“Even though vaccinated patients in this study showed elevated myocardial FDG uptake on PET/CT up to 180 days after vaccination, this could result from relatively minor inflammation and may not represent severe myocardial abnormalities,” they said.
The study was published by the Radiological Society of North America. Some authors disclosed grants from pharmaceutical companies, including Nihon Medi-Physics. The authors said they received no funding for the retrospective study.
Moderna and Pfizer didn’t respond to requests for comment. FDA Detects Serious Safety Signal for Covid Vaccine Among Kids
EditorialIn an editorial also published by Radiology, Dr. David Bluemke said the results of the study were compelling. He noted that researchers examined some potential confounders and the results held up. However, researchers didn’t test heart function.
“Unfortunately, no myocardial enzyme analysis was available, and cardiac function was not available. In addition, the authors did not scrutinize the oncologic histories and treatments of their patient groups,” wrote Dr. Bluemke, professor of radiology at the University of Wisconsin School of Medicine and Public Health and editor emeritus of the journal.
He also noted that retrospective studies are more prone to bias, with unknown factors, including why some patients receive a vaccine and some don’t. “The results are intriguing but unfortunately incomplete,” Dr. Bluemke said.
Heart inflammation is a known side effect of the Pfizer and Moderna vaccines. It can be deadly. The most common symptom is chest pain.
None of the patients analyzed in the study reported chest pain, although some reported noncardiac symptoms such as fever and a sore arm.
The study results “suggest that mild asymptomatic myocardial inflammation could be more common than we ever expected,” according to Dr. Bluemke. He said vaccine manufacturers may look to change their vaccines or delivery systems with the aim of reducing the inflammation. Others Weigh InDr. Sanjay Verma, an American cardiologist who wasn’t involved in the research, told The Epoch Times in an email that the increased FDG in vaccinated patients tested before and after receiving a vaccine “does suggest that vaccination rather than underlying inflammation alone is playing a causal role in the increased FDG uptake after vaccination.” He said the study adds to other research and his own experience with patients, showing the need for doctors to understand that heart problems after COVID-19 vaccination can result in symptoms other than chest pain, including fatigue and shortness of breath.
“It is imperative that medical professionals broaden their scope of what symptoms they identify as potentially related to heart damage after COVID-19 vaccination,” Dr. Verma said. Early detection means earlier treatment, which can lead to quicker recovery, according to the doctor.
Both Dr. Verma and Dr. Andrew Bostom, a U.S. heart expert who also reviewed the paper, said the findings were preliminary because there were no signs that the FDG levels resulted in health issues.
“If the investigators can show the PET findings predict hospitalizations for heart failure or cardiac arrhythmias or sudden cardiac death, upon prospective follow-up, that would [be] much more interesting,” Dr. Bostom told The Epoch Times via email. Retrospective studies examine medical records, while prospective studies track patients for a period of time.
The study went over scans performed in adult patients between November 2020 and March 2022. The population before exclusions was about 9,400. Researchers excluded many of the patients, including patients who received more than two doses of a vaccine, patients with a history of COVID-19, and patients who underwent cardiac surgery.
Dr. Nakahara didn’t respond to a request for comment. The researchers said one limitation of the study is that it was retrospective. “A prospective study would be needed to validate the findings of this study including comparisons with cardiac enzyme, cardiac functions and non-mRNA vaccination,” they wrote.
The Pfizer and Moderna vaccines use mRNA technology.
A prospective study of 54 participants, published in Radiology earlier this year, found increased FDG uptake in two COVID-vaccinated people who suffered acute myocarditis but normal levels in vaccinated people who didn’t. The study duration was only two months. FDG TestingThe FDG testing has, for years, been used to detect cardiac sarcoidosis, an inflammatory heart disease. It has increasingly been used to detect myocarditis and a related condition, pericarditis, in lieu of or with cardiac MRIs.
Some research has found that F-FDG testing produced results similar to the MRIs, although other papers have concluded that the testing was inferior.
The testing involves injecting a tracer, or a drug, and imaging with the PET scan to measure levels of fluorodeoxyglucose. CT scans are sometimes done to supplement the PET scans.
The testing can detect problems overlooked or unclear in other scans. It’s “much more sensitive than other imaging modalities like echocardiogram and cardiac MRI in identifying myocardial ischemia or injury,” Dr. Verma said.
The testing has been used in the past to detect heart inflammation in people who had COVID-19, in addition to the vaccinated people.
Zachary Stieber
Zachary Stieber is a senior reporter for The Epoch Times based in Maryland. He covers U.S. and world news. Contact Zachary at zack.stieber@epochtimes.com
|
|
They Suffered Myocarditis After COVID-19 Vaccination. Years Later, Some Still Haven’t Recovered.By Zachary Stieber, Lia Onely | 20September2023 Updated: 21September2023 https://www.theepochtimes.com/article/they-suffered-myocarditis-after-covid-19-vaccination-years-later-some-still-havent-recovered-5478652
Under pressure from the military and his mother, Jacob Cohen was feeling increasingly cornered.
Mr. Cohen did not want to receive a COVID-19 vaccine. He knew the shots had not been available for long. He was worried about their safety.
While Mr. Cohen initially resisted receiving a shot, he faced restrictions such as being forced to remain on base while vaccinated soldiers left. He was also pressured by military commanders, who scheduled a vaccination appointment for him and contacted his mother as part of a multipronged campaign.
“They told me, ‘Come on. It’s your mother. She’s crying. She’s worried. What wouldn’t you do for her?'” Mr. Cohen, who asked to be identified by a pseudonym because of concern about repercussions for going public, told The Epoch Times.
“I didn’t want to take the vaccine. I didn’t believe in it,” he said. But he wanted to appease his mother. “I would do anything for her.”
Mr. Cohen received his first shot, manufactured by Pfizer, on Sept. 22, 2021. He was 21.
Two weeks later, he was awakened by a sharp pain at 3 a.m.
“I felt like my heart was trying to get out of my chest,” Mr. Cohen said.
The soldier has felt pain before. “I never felt something like this,” he said.
Mr. Cohen went with a friend to the hospital, where he was placed in quarantine because he wasn’t fully vaccinated. Thirty minutes ticked by.
“I felt like it was the first time in my life I actually started seeing flashbacks of things that I did in my life—I felt like I was truly dying,” Mr. Cohen said.  U.S. Army soldiers prepare Pfizer COVID-19 vaccines at the Miami Dade College North Campus in North Miami on March 9, 2021. (Joe Raedle/Getty Images
Doctors finally came in and ran tests. They diagnosed Mr. Cohen with perimyocarditis, or inflammation of the heart muscle and the tissue around the heart.
They said Mr. Cohen was lucky. If he had come just a little later, he would have needed open heart surgery.
He spent three days in the hospital, taking medication and pills. When he was discharged, he was told not to engage in any physical activity for at least six months. He also needed to report for regular checkups and take a pill every day.
Six months after leaving the hospital, Mr. Cohen’s cardiac MRI showed concerning results. His heart still hadn’t recovered.
Doctors gave him more pills.
“They told me maybe I will need them for the rest of my life,” Mr. Cohen said.
The military marked him as unable to serve for the rest of his life, and released him.
To this day, he suffers.
“I’ve been feeling, I’m not sure if it’s trauma or something, but it feels sometimes like a sting there, a short sharp pain,” Mr. Cohen said.  I did a lot of physical things, which now I can’t afford… to do amymore. – Jacob Cohen (pseudonym). military personnel He’s also unable to do all he used to do before.
“I was training. I was playing soccer. I did a lot of physical things, which now I can’t afford … to do anymore,” Mr. Cohen said. ‘Continued Pain’Dr. Adam Hirschfeld was among the first people to receive a COVID-19 vaccine in the United States
The orthopedic surgeon was motivated by a desire to prevent his patients from becoming sick.
“I didn’t want to put any of my patients at risk,” Dr. Hirschfeld told The Epoch Times.
He received a Moderna primary series, composed of two doses, in January 2021. He was 36.
Three days after the second shot, Dr. Hirschfeld felt discomfort in his chest and numbness in his left arm.
A cardiac MRI confirmed evidence of heart inflammation. Dr. Hirschfeld was prescribed medicine and discharged two days later.
Dr. Hirschfeld has since undergone about a dozen electrocardiograms, another half a dozen echocardiograms, and a follow-up cardiac MRI.
“I went from being completely healthy—no issues, no medications—to seeing 10 different doctors in the blink of an eye,” Dr. Hirschfeld said.
The follow-up MRI, conducted about 18 months after the vaccinations, showed normal cardiac function.  I went from being completely healthy-no issues, no medications-to seeing 10 different doctors in the blink of an eye. – Dr. Adam hirschfeld, orthopedic surgeon But Dr. Hirschfeld still experiences pain.
“I have continued chest pain on the right side, and then I have neuropathic type pains in my neck and shoulder areas,” he told The Epoch Times. “I have it when I wake up, and it’s there when I go to sleep.”
The suffering affects the doctor physically and mentally.
“Having chest pain every day for two and a half years is very disconcerting,” he said.
Pfizer and Moderna didn’t respond to requests for comment. Shots Cleared; Cases AppearMr. Cohen lives in Israel. Dr. Hirschfeld lives in the United States.
The first myocarditis cases after COVID-19 vaccination were reported in those countries in January 2021. Only a few weeks had elapsed since authorities cleared and recommended the shots for large portions of the population, including many young, healthy people.  A man receives the first dose of a Moderna COVID-19 vaccine in Meitar, Israel, on March 9, 2021. (Amir Levy/Getty Images)
At first, authorities hid reports of myocarditis from the public. Israel first acknowledged there was a likely link between the shots and the inflammation. The United States finally followed in June 2021, when the U.S. Centers for Disease Control and Prevention (CDC) said there was a “likely association.”
Even after the association was made public, officials and many experts claimed that the myocarditis cases were mild. Most patients were hospitalized, authorities acknowledged, but they said patients could expect to recover without treatment and with rest.
The myocarditis is “rare but mild,” Dr. Rochelle Walensky, the CDC’s director at the time, said on “Good Morning America” on June 24, 2021.
Dr. Walensky said the cases were “self-limited,” or didn’t require treatment to resolve.  Then-Centers for Disease Control and Prevention Director Dr. Rochelle Walensky speaks to reporters at a COVID-19 mass vaccination site at Hynes Convention Center in Boston on March 30, 2021. (Erin Clark-Pool/Getty Images)
Dr. Jeremy Faust, editor-in-chief of MedPage Today and a teacher at Harvard Medical School, on Twitter two days later described the cases as “self-limited troponinemia,” or elevated troponin levels that would resolve on their own. Troponin is a protein in the heart that’s a marker of heart injury.
Those claims were already wrong at the time, based on case reports alone.
A previously healthy 24-year-old man in Massachusetts, for example, experienced chest pain so serious that he went to an emergency department, doctors reported on May 18, 2021. He was eventually discharged with a prescription for a beta-blocker and anti-inflammatory drugs and told not to engage in strenuous activity for three months.
Another early case involved a previously healthy 16-year-old boy in California who experienced “stabbing chest pain” and went to the emergency department for help. He described the pain as 6 to 8 on a scale of 1 to 10. The symptoms prompted doctors to admit him to intensive care. He spent six days in the hospital before being discharged.
Like many early case reports, no follow-up data were reported, making it impossible to say that the cases had fully resolved.
“Unless you’ve experienced it individually, you can’t tell somebody that their case was mild,” Dr. Hirschfeld said. “If you have elevated troponin, that’s your cardiac muscle breaking down.
“That’s something that’s permanent. And so to tell me that my cardiac muscle breaking down is mild is pretty insulting.”  Unless you’ve experienced it individually, you can’t tell somebody that their case was mild. – – Dr. Adam Hirschfeld, orthopedic surgeon Signs of persistent symptoms appeared in the literature before long. U.S. military researchers, for instance, stated on June 29, 2021, that seven of 23 patients continued to have chest discomfort weeks or even months later. Dire outcomes were known even earlier. Two deaths were reported to U.S. authorities in February 2021, while another two were reported in Israel in the spring. Both of the Israelis who died were previously young and healthy. Professional Biker AffectedKyle Warner was a professional mountain bike racer when he received his first COVID-19 vaccine in May 2021. He completed a primary series the following month.
Mr. Warner, who lives in the western United States, teaches older people and wanted to protect them from COVID-19. The CDC and others promoted the idea that the vaccines curbed or even prevented transmission based on observational data.
“The sentiment was these are safe and effective. If you get them, you don’t need to wear a mask anymore, and you can’t transmit COVID or catch COVID,” Mr. Warner told The Epoch Times. “I spend quite a bit of time around older people and help them learn.
“I wasn’t necessarily afraid of COVID myself. Not that I did respect it, but I wasn’t worried it was going to kill me,” he added. “But I was worried about getting someone else sick, especially when I’m with our older clients.”  A woman receives a dose of the COVID-19 vaccine at the Corona High School gymnasium in Corona, Calif., on Jan.15, 2021. (Frederic J. Brown/AFP via Getty Images)
Mr. Warner was diagnosed with myopericarditis after COVID-19 vaccination and was hospitalized.
After being discharged, Mr. Warner was bedridden for weeks.
“There’s points where I was unable to even get up out of bed without passing out or blacking out,” Mr. Warner told The Epoch Times. “It was really eye-opening. I felt like I went from being 28 years old to being 88 years old.”
Mr. Warner was diagnosed with myopericarditis and two other conditions—postural orthostatic tachycardia syndrome and mast cell activation syndrome—that others have also been diagnosed with following COVID-19 vaccination.  I felt like I went from being 29 years old to being 88 years old. – Kyle Warner, professional mountain bike racer Hyperbaric oxygen, which has relieved some of Dr. Hirschfeld’s pain, helped bring Mr. Warner’s energy levels back up.
But the cyclist, who didn’t ride again until February 2022, still struggles with pain, especially when he exercises in the summer.
Mr. Warner utilizes a heart rate monitor, which he became familiar with in his racing career.
During a recent ride, Mr. Warner pushed himself, trying his hardest for four minutes. That sent his heart rate up to 189 beats per minute—the highest since the injury.
“I did OK, but then the next few weeks, I had a kind of a lingering chest pain and tightness. And about four days after, it was pretty significant where I was having a hard time sleeping and my heart felt like it was palpitating every once in a while, and then—even more than a week later—I still had a little bit of chest tightness and pain,” Mr. Warner said.
“It kind of scared me because it’s been well over a year since my last treatment with hyperbaric and I’m still dealing with it. And when I do try to push myself harder, then I have to pay for the next few days to a week.
“Back in the day, I would be able to do that with no problem at all.”
Doctors who have spoken to Mr. Warner have told him that when his heart becomes stressed, it signals his immune system to attack and inflame it.
He tries to keep his heart rate under 160 beats per minute. A man monitors his heart rate using a fitness tracker. (ThamKC/Shutterstock)
14-Year-Old Rushed to HospitalAiden Ekanayake woke up in the middle of the night.
“Every breath deeper in was like knives in my chest,” Aiden, who is from Georgia, said during a podcast appearance.
It was June 12, 2021, two days after Aiden received a second shot of Pfizer’s vaccine. He was 14.
Aiden was able to fall asleep through shallow breathing, but was soon awakened. He went to his mother, who rushed him to the hospital.  Every breath deeper in was like knives in my chest. – Aiden Ekanayake, student Tests revealed abnormalities. Aiden was taken to the acute cardiac unit, where more tests confirmed that the vaccine was the cause.
Aiden spent four days in the hospital. After being discharged, he was inactive for more than four months.
“I don’t know where they get this ‘two days and you’re done, you’re good.’ That’s a crock of [expletive],” Emily Ekanayake, Aiden’s mother, told The Epoch Times.
Ms. Ekanayake had read early studies from Israel that found an elevated risk for myocarditis among young males who had received the Pfizer vaccine, but concluded with her son that the benefits of the vaccine outweighed the risks.
“I was really scared of COVID,” Ms. Ekanayake said.
Aiden said he wanted to get vaccinated to help protect himself and his brother, both of whom have asthma.
Aiden’s doctor also recommended the shot. Shortly before Aiden was vaccinated, the CDC director said the agency found no safety signal for myocarditis. U.S. officials cleared and recommended the vaccine to virtually all children aged 12 to 15, after initially only making it available to those 16 and older.  Aiden Ekanayake in a hospital in June 2021. (Courtesy of Emily Ekanayake)
Aiden eventually resumed exercise after being cleared by a cardiopulmonary stress test.
The result of the test was “probably more like that of an old man,” Ms. Ekanayake said. “His CO2 was low. He wasn’t able to run much. He’s got a lot of work in that way to go still. But he does like walking.
“I still worry about strenuous activity. I can’t help it. I don’t know that that will ever go away.” ‘Half a Human Being’Alon was a competitive swimmer who trained every single day before he received his Pfizer vaccine.
But in addition to the round trip to get to the pool, the Israeli boy needed to stand in line to take a test for COVID-19.
School also was an issue. Fellow students would often get sick, triggering a quarantine of those who weren’t vaccinated.  It’s like putting a child in prison for doing no wrong. – Mother of Alon, vaccinated child “There was no chance to arrive to school and not be informed the next day that someone is sick and you [need to] be in quarantine,” Alon’s mother, who spoke on condition of anonymity due to fear of professional repercussions, told The Epoch Times. “It’s impossible. It’s like putting a child in prison for doing no wrong.”
Alon’s mother saw vaccinated people become sick despite the vaccine, erasing her belief that the shot protected people. But she heard little about possible side effects and decided that the benefits, including keeping her son in school, meant he should receive the shot.
“He was tired of the quarantines and tests,” she said.  Students are tested for COVID-19 at Brandeis Elementary School in Louisville, Ky., on Aug. 17, 2021. (Jon Cherry/Getty Images)
The first shot was injected on Dec. 3, 2021; the second shot was on Dec. 24, 2021. Alon was 9.
A few days later, Alon fell into a deep sleep.
“It was scary,” Alon’s mother said.
Doctors ran tests, including checking his heart. They couldn’t discern what was awry.
“The child is not functioning,” Alon’s mother said. “He was like half a human for the whole month.”
The breakthrough came when Alon said, “My heart hurts.” Fresh testing revealed myocarditis. It was induced by the vaccination, doctors concluded.
Alon spent the night at the hospital before being discharged. He returned a week later with chest pain. Tests showed normalization.
Alon suffered from other problems over the months that followed. He lost his sight. His leg swelled. His lymph nodes became enlarged.
Follow-up visits found no heart problems. The other symptoms eventually resolved and Alon was cleared to resume sports. He plays for hours each day. But nearly two years later, he still suffers.
“He has periods when his heart hurts,” Alon’s mother said. “Sometimes for a few months, everything is fine. And then suddenly, it comes back.”
She has opted to take her son to the doctor only when emergencies arise. Any time he sees a doctor, he becomes sick. And he refuses to take any more blood tests.
“Maybe it is a sore muscle there. The heart is normal and suddenly, it is very tight for a few seconds,” Alon’s mother said. “It goes away. We avoid tests of any sort. If I don’t feel it’s life and death, I don’t take him to the doctor.” Worst Pain in His LifeBen Cutler loved to go to the gym. He worked out five days a week.
Because he didn’t want to become infected by the new Omicron variant, Mr. Cutler received a Moderna booster shot on Dec. 14, 2021. He was 26.
The next day, Mr. Cutler began to experience symptoms such as fatigue. He went to sleep early, but at 2:30 a.m., he was startled awake.  Ben Cutler on Nov. 21, 2021, before he received a Pfizer-BioNTech COVID-19 booster shot. (Courtesy of Ben Cutler)
 Ben Cutler in a hospital in Massachusetts on Dec. 19, 2021, after suffering COVID-19-vaccine-induced myopericarditis. (Courtesy of Ben Cutler)
“I woke up and have never felt so terrible in my life,” Mr. Cutler wrote in a summary of his experience.
After several days of trying to sleep the pain away, a family member convinced the Massachusetts resident to go to the hospital.
Doctors ran tests and found troponin-T levels almost 90 times the normal maximum levels.
Mr. Cutler was diagnosed with myopericarditis. He was eventually discharged, but his ordeal wasn’t over.
“It was good that I could work from home. And I could start working at 7 or 8 a.m. and then work until like 2ish and then just lay on my couch for like seven hours,” Mr. Cutler told The Epoch Times.
 Ben Cutler estimated that he lost 25 pounds while spending hundreds of hours in pain on his couch in extreme pain. Mr. Cutler estimated he spent hundreds of hours in pain on his couch. His pain was often 5 on a scale of 5. He lost 25 pounds.
A 10-minute walk to the grocery store, Mr. Cutler said, would have been the only exercise he could manage in a day. He described having to “budget” his energy.
After about two months, his condition started to improve. The pain dropped to 3s on some days. Then 2s. Then zeros.
By the end of April 2022, Mr. Cutler was able to begin lifting weights again. A follow-up cardiac MRI revealed a small fibrosis, or scar, but he feels he has recovered.
“I haven’t been having any major issues,” he said. “Everything’s pretty good.” Evidence BuildsThe stories bolster the growing body of evidence that has found a significant portion of people who suffer vaccine-induced myocarditis are affected for months or years, if they survive.
U.S. researchers who followed up with 15 children hospitalized with myocarditis after COVID-19 vaccination revealed on Aug. 10, 2021, that four of the patients had “persistent symptoms.” Other U.S. researchers announced on Nov. 1, 2021, that seven of 54 young patients who suffered myocarditis after vaccination still experienced symptoms, including chest pain.
 47% Nearly half of myocarditis patients who responded to a U.S. government survey said they continued to experience symptoms months after COVID-19 vaccination. Nearly half of myocarditis patients who responded to a U.S. government survey said that months after COVID-19 vaccination, they continued to experience symptoms, including chest pain, government researchers said on Sept. 21, 2022. Meanwhile, 35 percent of 28 young myocarditis patients followed up with at least 61 days after COVID-19 vaccination reported continued symptoms such as shortness of breath, Hong Kong researchers said on Sept. 23, 2022.
“Although post-COVID-19 vaccination myocarditis has a favorable prognosis and is considered curable, it may leave abnormalities in the myocardium, as observed in this case; it may therefore be premature to declare it as a complication with a good prognosis,” Japanese researchers said in 2022.
More recent data have shown that some patients still haven’t recovered.
That includes 23 percent of 60 people who told the CDC that at least one year after being diagnosed with myocarditis, they were still experiencing chest pain.
Other papers have found that even when symptoms abate, follow-up testing reveals abnormalities.  Cars line up for a mass COVID-19 vaccination event in Denver on Janu. 30, 2021. (Michael Ciaglo/Getty Images)
Heart scars were detected in cardiac MRIs conducted seven to eight months after the myocarditis diagnoses, Israeli researchers said on March 23, 2022. U.S. researchers described similar results in a study published around the same time. Other U.S. researchers who imaged 15 adolescents at least 76 days after they were discharged from a hospital found persistent late gadolinium enhancement in 80 percent of the patients.
Researchers often use abnormal levels of late gadolinium enhancement as an indication of heart scarring.
In myocarditis cases before the pandemic, the enhancement was often a sign of poor outcomes such as heart transplantation or death.
“It’s going to be a small percentage of the people that recovered from myocarditis, but some of them could be in for longer-term problems and morbidity, and some of them may develop actual disability,” Dr. Andrew Bostom, a U.S. heart expert, told The Epoch Times.
While most patients experienced “mild myocarditis, which is mostly gone, it’s true that scars can remain, because it’s an inflammation of the heart muscle,” Dr. Yehuda Adler, a member of the Israeli Ministry of Health’s National Council for Prevention and Treatment of Cardiovascular Diseases, told The Epoch Times. “I’m definitely following these people even today, two years later, and I’ll continue to follow them.”
Not all patients have persistent symptoms or abnormalities. Some have seen a full resolution of their symptoms, combined with no abnormal signs in follow-up testing.
Dr. Rabea Asleh, director of the heart failure unit and the cardiovascular research center at the Hadassah University Medical Center in Jerusalem, said his team is also following patients to make sure they’re OK.
He told The Epoch Times that all but one of his patients have stopped experiencing symptoms.
“If this has any clinical significance regarding the flare-up of the disease later on or the deterioration in function after a few years, we do not know,” Dr. Asleh said, “but deterioration in function after a few years is unlikely.”
Dr. Bostom said he wasn’t so sure. “One thing that I’m certain of is that the jury is out,” he said. “We need to collect a lot more information and see how people are really doing long term, particularly the young people.” Questionable PressureMany young people received COVID-19 vaccines under pressure, such as Mr. Cohen.
Israeli military authorities punished the unvaccinated with actions ranging from taking away their leave to making them wear a special vest and isolate in their quarters.  Military personnel receive a dose of the COVID-19 vaccine at a military base in Rishon Lezion, Israel, on Dec. 28, 2020. (Jack Guez/AFP via Getty Images)
“This is a population of young and healthy soldiers, in whom COVID is mild and transient, and there is no justified reason to vaccinate them,” Dr. Yoav Yehezkelli, a specialist in internal medicine and medical management, said on Facebook. “Vaccinating the soldiers was not only folly but a lack of professionalism and a violation of medical ethics.”
 This is a population of young and healthy soldiers, in whom COVID is mild and transient, and there is no justified reason to vaccinate them. – Yoav Yehezkeilli, specialist
Others, like Alon, faced repeated interruptions to their daily lives if they didn’t receive a vaccine, despite evidence suggesting that post-infection immunity is broad and superior to that from vaccination.
CDC studies later found that the immunity that develops following recovery, known as natural immunity, was better than vaccination against the Delta and Omicron virus variants.
Top U.S. officials made false claims about vaccine effectiveness, such as claiming vaccinated people couldn’t become sick or transmit the virus, in their bid to convince fence-sitters to get vaccinated.  Dr. Jay Bhattacharya, professor of health policy at Stanford University’s School of Medicine. (Tal Atzmon/The Epoch Times)
“You can’t make that logical leap even in December of 2020. And yet, they made that logical leap,” Dr. Jay Bhattacharya, professor of health policy at Stanford University’s School of Medicine, told EpochTV’s “American Thought Leaders.”
“They premised their policy recommendations—the vaccine passports, the mandates, the coercion, and also the gaslighting of people who are actually vaccine-injured, on this idea that we have to get a sufficient fraction of the population vaccinated for the disease to go away.”
The hype around the vaccines led to a number of U.S. universities to mandate them, even after researchers concluded that booster mandates were unethical, in part because they were associated with more serious adverse events than hospitalizations caused. The federal government also imposed mandates on the military, workers, contractors, and private health care facilities.
The White House has defended the mandates.
“Our administration’s vaccination requirements helped ensure the safety of workers in critical workforces including those in the healthcare and education sectors, protecting themselves and the populations they serve, and strengthening their ability to provide services without disruptions to operations,” it said in a recent statement. Common Symptoms and TreatmentsNearly all people who develop myocarditis after COVID-19 vaccination suffer from chest pain, doctors have found.
A meta-analysis of reports describing 200 cases, for instance, found that 98 percent of patients presented with chest pain. Fever and difficulty breathing were also common symptoms.
Patients often suffer symptoms within a week of vaccination, according to case reports, surveillance databases, and patients.
Early detection and treatment can be critical to prevent further deterioration. Exercise restrictions are imposed on most patients until they pass a cardiac stress test.
The point of the test is to detect lingering problems in a controlled setting, in which the patient exercises at less than maximum capacity, Dr. Anish Koka, a U.S. cardiologist, told The Epoch Times. Problems detected on the test may preclude participation in competitive sports and may require invasive therapies such as defibrillator placement.
Some health officials and doctors have said the myocarditis resolves without treatment, but many patients have received drugs.
Colchicine, typically used to treat gout, has been favored by many doctors.
Mr. Cohen was initially prescribed colchicine. He was directed later to daily take Tritace, an angiotensin-converting enzyme inhibitor that’s meant to treat hypertension following serious problems such as heart failure.
Mr. Cutler took aspirin for two weeks. He replaced colchicine with ibuprofen after experiencing back pain.
Other treatments include intravenous immunoglobulin, a pooled antibody; beta-blockers; anti-inflammatory medications such as methylprednisolone; and rampiril, another angiotensin-converting enzyme inhibitor.  Treatments for myocarditis include methylprednisolone. (Felipe Caparros, GeorgiosKostomitsopoulos, George Martin Studio/Shutterstock)
 Treatments for myocarditis include colchicine. (Felipe Caparros, GeorgiosKostomitsopoulos, George Martin Studio/Shutterstock)
 Treatments for myocarditis include ibuprofen. (Felipe Caparros, GeorgiosKostomitsopoulos, George Martin Studio/Shutterstock)
‘Ignored’Several common themes link the myocarditis patients who are speaking out. That includes the feeling that they were tricked into receiving the shots.
“You start to realize that basically the authorities, first of all, they knew about these possible side effects. They just chose not to disclose it, or disclose it only in the few websites in the small letters,” Mr. Cohen said.
Mr. Warner recounted growing up on welfare and coming to see the government as being there to help him. He now views parts of the government as corrupted by financial incentives, including the kickbacks it allegedly received from Moderna.
Patients also feel abandoned.  You Start to realize that basically the authoritites first of all, they knew about these possible side effects. They just chose not to disclose it. – Jacob Cohen (pseudonym). military personnel “A lot of us are still dealing with significant issues that I think are being ignored,” Dr. Hirschfeld said.
It hasn’t helped that U.S. authorities, who have aggressively promoted the vaccines, have refused to provide compensation to many sufferers or otherwise assist them.
Just three people who suffered post-vaccination myocarditis have been compensated by U.S. authorities, who are responsible for compensation because the vaccine manufacturers are shielded from liability. The highest payout was just $3,957.66.
Both Ms. Ekanayake and Mr. Cutler applied for compensation, but still haven’t heard back. While the bulk of Aiden’s medical bills were covered by insurance, his parents have still had to pay close to $10,000 out of pocket. Mr. Cutler paid about $5,000 due to high deductibles.
An enormous backlog of applications remains, and some who have been diagnosed with vaccine injuries have been denied.
The myocarditis patients largely spoke about receiving the support of family and friends as they recovered. But not all.
“I was disowned by many of my friends for speaking out about this early on,” Mr. Warner said. “It’s been interesting to see so many of them come back around and apologize to me.”
|
|
Nearly 1 in 3 COVID-19 Vaccine Recipients Suffered Neurological Side Effects: StudyThe people included in the study suffered from headaches, tremors, muscle spasms, insomnia, sleepiness, vertigo, and difficulty in concentration.By Naveen Athrappully
Almost a third of individuals who received a COVID-19 vaccine suffered from neurological complications including tremors, insomnia, and muscle spasms, according to a recent study published in the journal Vaccines.
study analyzed 19,096 people who received COVID-19 vaccines in Italy in July 2021, out of which 15,368 had taken the Pfizer vaccine, 2,077 had taken the Moderna version, and 1,651 took the AstraZeneca version.
While both Pfizer and Moderna are mRNA vaccines, AstraZeneca, being an adenovirus vaccine, uses a different mechanism to trigger the immune response.
The study found that about 31.2 percent of vaccinated individuals developed post-vaccination neurological complications, particularly among those injected with the AstraZeneca jab. Different vaccines had a different “neurological risk profile.”
The neurological risk profile of the AstraZeneca vaccine included headaches, tremors, muscle spasms, insomnia, and tinnitus, while the risk profile of the Moderna vaccine included sleepiness, vertigo, diplopia (double vision), paresthesia (a feeling of numbness or itching on the skin), taste and smell alterations, and dysphonia (hoarseness or loss of normal voice). None of the subjects were hospitalized or died.
As to Pfizer vaccines, researchers found “an increased risk” of cognitive fog or difficulty in concentration. AstraZeneca RisksMore than 53 percent of individuals who took an AstraZeneca shot suffered from headaches, which usually lasted for one day. Over 13 percent developed tremors, which typically reverted after a day as well.
Insomnia was reported among 5.8 percent of AstraZeneca recipients. However, the study notes that researchers were unsure whether the individuals actually developed insomnia or had a “misperception of their sleep quality due to vaccination stress.”
Tinnitus was reported by 2.7 percent of the people who took AstraZeneca shots. Tinnitus is a condition in which an individual hears ringing or other noises which are not caused by an external sound.
All these health complications had a higher risk of occurring after taking the first dose of the vaccine. The study speculated that complications related to the AstraZeneca vaccine are attributable to two factors. “Firstly, the nature of the vaccine, which is a modified adenovirus vector that results in significant and persistent systemic immune activation; secondly, individual vulnerability related to a predisposing biology.”
Delve into the Untold Stories Surrounding COVID-19 Vaccines | CrossroadsModerna and Pfizer RisksSleepiness was found in 39.7 percent of those who took Moderna jabs, with the condition usually lasting for a week. It suggested that there “could be a strict relationship between the development of sleepiness and immune responses to vaccine/infection.”
The study cited a “fascinating hypothesis” which suggests that influenza vaccines may lead to “the selective immune-mediated destruction of orexin-producing neurons, which is T-cell-mediated neuronal damage, thus triggering narcolepsy.”
Narcolepsy is a condition in which the brain is unable to control the ability to sleep or stay awake.
“Considering that the same can occur for COVID-19 vaccines, future investigations monitoring the new-onset hypersomnia findings in vulnerable individuals are urgently needed.”
Hypersomnia is the inability to stay awake and alert during the daytime, even though the person may have had plenty of sleep during the night.
About 15.9 percent of people who received Moderna shots had vertigo, a sensation which makes the individual feel that they or their surrounding environment is moving or spinning. It typically lasted for a day.
Paresthesia—a feeling of numbness or itching on the skin for no apparent reason—was reported in 14.5 percent of Moderna vaccine recipients, which went away after a day.
Among the people who received a Moderna jab, 2.7 percent reported diplopia, also known as double vision, which also lasted for about a day. “Symptomatic people showed an increased risk to develop diplopia after the second dose, as if a reactivation of the immune response was necessary to trigger diplopia.”
Meanwhile, about 6.4 percent of Pfizer vaccine recipients reported suffering from cognitive fog, with the condition usually reversing in a week.
“Brain fog is a type of cognitive impairment that presents as a ‘foggy brain state’, including a lack of intellectual clarity, difficulty with concentration, mental fatigue and anxiety,” the study said.
“Hypotheses including systemic inflammation crossing the blood–brain barrier, neuroinflammation after viral infection leads and microglial activation are emerging as explanations of this phenomenon in COVID-19 patients. An alternative speculation is that symptomatic people may have a subclinical cognitive dysfunction before vaccination, and that vaccination is a trigger.” Females Highly AffectedThe study found that females faced an “increased risk of developing neurological complications” following COVID-19 vaccination. “Our findings are in line with those of a recent study that revealed that several factors, including the female sex, were associated with greater odds of adverse effects,” it said.
The researchers suggested that greater female susceptibility to the vaccines’ neurological complications may be due to “genetic and hormonal factors.”
Females have two X chromosomes while males have one X chromosome and one Y chromosome. As the X chromosome “contains the most prominent immune-related genes in the human genome,” it can also cause “stronger inflammatory immune responses,” the study said.
Moreover, a primary female sex steroid called estradiol triggers a specific immunity process to produce “antibodies against infections.”
The study also raised concerns about comorbidities. In medical parlance, comorbidity describes the existence of more than one disease or condition in a body at the same time, which may or may not interact with one another.
“The evidence that immune system dysfunctions (allergies/immunodeficiency disorders) are frequently reported in our symptomatic group is more than a chance occurrence,” researchers said.
Comorbidities were present in 47.6 percent of the AstraZeneca vaccine recipients, 38.8 percent of those who took Moderna jabs, and 41.5 percent of individuals who received Pfizer shots, the study said.
In the AstraZeneca group, both allergies and non-neurological diseases were reported. “A history of antitumoral and anticoagulant drugs was more frequent in this population,” the study said.
Among Moderna and Pfizer recipients, allergies were “more frequently” observed. While some people who took Moderna had a prior history of neurological diseases and transfusions as well as previous COVID-19 infection, those who received Pfizer vaccines had a history of immunodeficiency disorders.
Even though the study detailed neurological complications arising from COVID-19 vaccination, it admitted to certain limitations.
“Firstly, our results should be interpreted with caution because of a possible overestimation of neurological events resulting from the self-reported symptoms,” it said.
“Secondly, we evaluated the risks associated with the first and second doses of the vaccine; however, the data concerning the second dose were limited, thus representing a potential bias in the study.”
While admitting its limitations, the study concluded that “clinicians should be aware that several neurological complications may commonly occur after COVID-19 vaccines.”
“Caution should be used when administering COVID-19 vaccines to vulnerable people, such as to those who suffer from allergies,” the study stated. “We strongly believe that our findings are relevant for public health regarding the safety of vaccines in a large cohort.”
The Epoch Times reached out to Moderna, Pfizer, and AstraZeneca for comment. Additional Neurological FindingsCardiologist Dr. Peter McCullough wrote about the study discussing neurological effects following COVID shots in an article on Substack.
“A shocking 31.2 percent of respondents to this large dataset sustained neurologic injury after two injections with verified data in health registries,” he wrote. “Most of the risk estimates indicate the safety profile is unacceptable. It is alarming that all neurological societies to date still recommend COVID-19 vaccines and none have issued safety warnings on the products.”
Dr. McCullough explained that an excess risk of 20 percent or greater is considered “clinically important.” Multiple other studies have found evidence of COVID-19 vaccines being linked to neurological complications. Back in October 2021, a study published in the Neurological Sciences journal stated that the “most devastating neurological post-vaccination complication is cerebral venous sinus thrombosis (CVST).”
CVST occurs when a blood clot develops in the venous sinuses of the brain. This blocks the blood from draining out of the brain, eventually resulting in the blood leaking into brain tissues and forming a hemorrhage, according to Johns Hopkins Medicine.
The study found that CVST was “frequently reported in females of childbearing age,” generally among those who took an adenovector vaccine. Individuals who received mRNA vaccination were reported to have Bell’s palsy, in which facial muscles weaken or enter into paralysis.
A November 2022 study in Current Neurology and Neuroscience Reports made similar findings, stating that there is “a greater than expected occurrence of severe neurological adverse events.”
Dr. McCullough cited this study in an article the following month. “Because the vaccines contain lipid nanoparticles loaded with genetic material that code for the damaging Spike protein, each patient faces a Russian Roulette of whether or not the nervous system will be hemodynamically showered with the damaging vaccine particles,” he wrote.
Despite studies suggesting the risk of medical complications, some experts continue to advise people to get COVID-19 jabs. According to John Hopkins Medicine, both Pfizer and Moderna are “highly effective in preventing serious disease, hospitalization, and death from COVID-19.”
It recommended people to get a COVID-19 shot as “we believe that their benefits outweigh their risks,” Johns Hopkins Medicine said.
According to a position statement from the American Academy of Neurology (AAN) issued in 2021, the organization recommended COVID-19 vaccine mandates for health care employees and supported vaccinations for children under the age of 12.
Naveen Athrappully |
|
Young adults who took 4 COVID vaccines are 256% more likely to die, especially from TURBO CANCERS03December2023 // Lance D Johnson // https://www.naturalnews.com/2023-12-03-young-adults-four-vaccines-256-percent-die.html 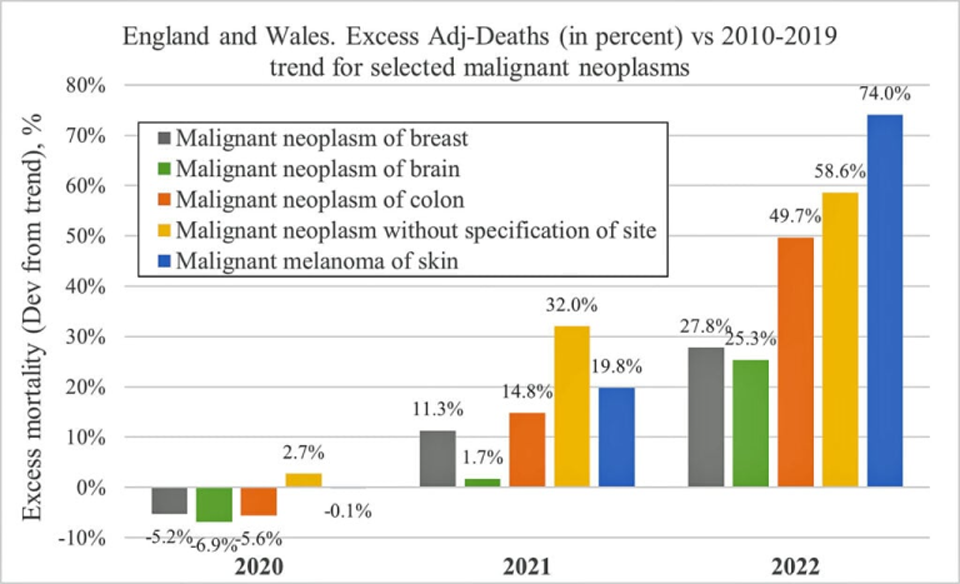 England and Wales Excess Adj-deaths vs 2010-2019 trend for Cancer The Office for National Statistics (ONS), the official reporting department of the United Kingdom, quietly published a data set that shows appalling mortality rates in young adults who took four Wuhan coronavirus (COVID-19) vaccines. The ONS data tracks deaths by vaccination status from April 1, 2021, to May 31, 2023. From January to May 2023, young adults aged 18 to 39 who were vaccinated four times up until that point were 256 percent more likely to die compared to their unvaccinated peers. In February 2023, the quadruple vaccinated were 318 percent more likely to die of any cause compared to unvaccinated people.
Cancer deaths skyrocket in young adults across the UK since COVID jab rolloutOne of the most alarming trends is skyrocketing cancer rates among young people. Fatal cancer rates exploded among U.K. teenagers and young adults who were vaccinated with spike protein mRNA. The 2022 ONS data shows a sudden rise in cancer deaths for the 15 to 44 age group. These cancer rates are well above the norms established from 2010-2019. They include:
England and Wales Excess Adj-deaths vs 2010-2019 trend for Cancer
Dr. Harvey Risch, a professor emeritus of epidemiology in the Department of Epidemiology and Public Health at the Yale School of Public Health and the Yale School of Medicine has noticed the alarming trend. He said that the number of “turbo cancers” is skyrocketing ever since the launch of Operation Warp Speed.
“What clinicians have been seeing is very strange things,” said Risch during an interview for EpochTV. “For example, 25-year-olds with colon cancer, who don’t have family histories of the disease – that’s basically impossible along the known paradigm for how colon cancer works – and other long-latency cancers that they’re seeing in very young people.”
Risch and his colleagues are seeing young people suffer through re-manifestation of cancers that usually take many years to form after they had been surgically removed.
“Those are the initial signals that we’ve been seeing, and because these cancers have been occurring to people who were too young to get them, basically, compared to the normal way it works, they’ve been designated as turbo cancers,” Risch explained.
Mortality rates skyrocket for young people who took 4 COVID jabsIn January 2023, the mortality rate per 100,000 person-years was 31.1 for the unvaccinated cohort. For individuals who took one COVID jab, mortality rates were much higher – 53.3 per 100,000 person-years. For the quadruple vaccinated, the rate was a shocking 106 per 100,000 person-years.
The average mortality rate per 100,000 person years from January to May was 26.56 for unvaccinated young adults and 94.58 per 100,000 person years for quadruple vaccinated young adults – a stark contrast. 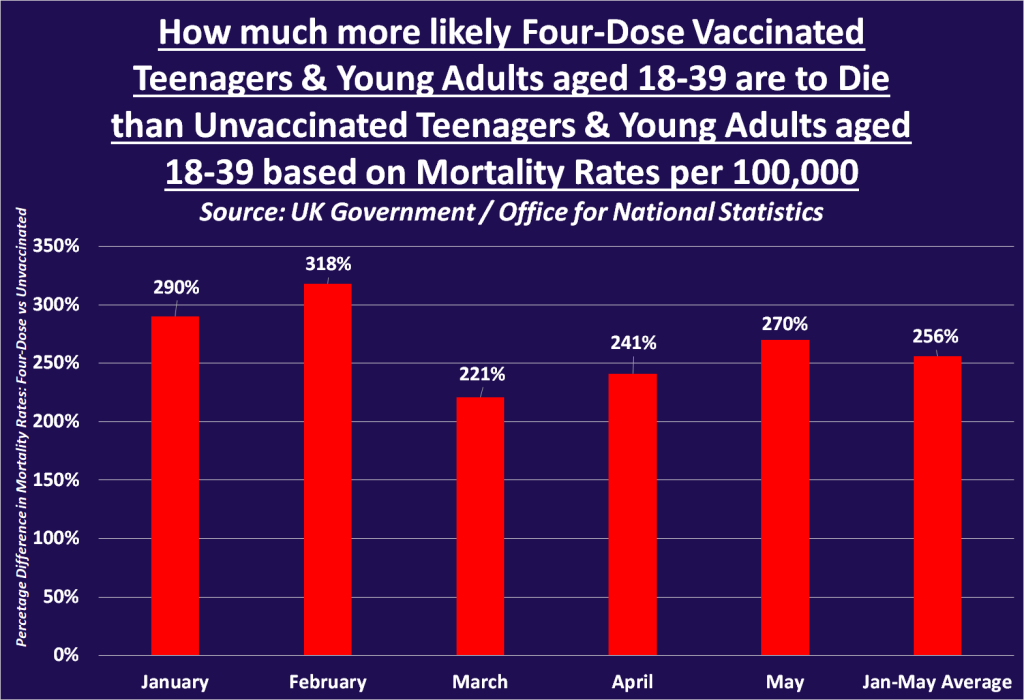 How much more likely 4 Dose Vaccinated 18-39 Die
A similar pattern was observed for adults aged 40 to 49. For every single month since the beginning of 2023, adults in this age group who were vaccinated with one or four doses were significantly more likely to die than their unvaccinated peers. January 2023 mortality rates were the worst for individuals who received either one or four COVID jabs, with a mortality rate per 100,000 of 411.3 and 258.5, respectively. In contrast, the unvaccinated saw a mortality rate of just 144.5 per 100,000.
The unvaccinated, having withstood aggressive coercion, abuse, and threats to their lives and livelihoods, are faring the best over the long haul, even after putting up with the stress, the lies, and abuse for the past three years. 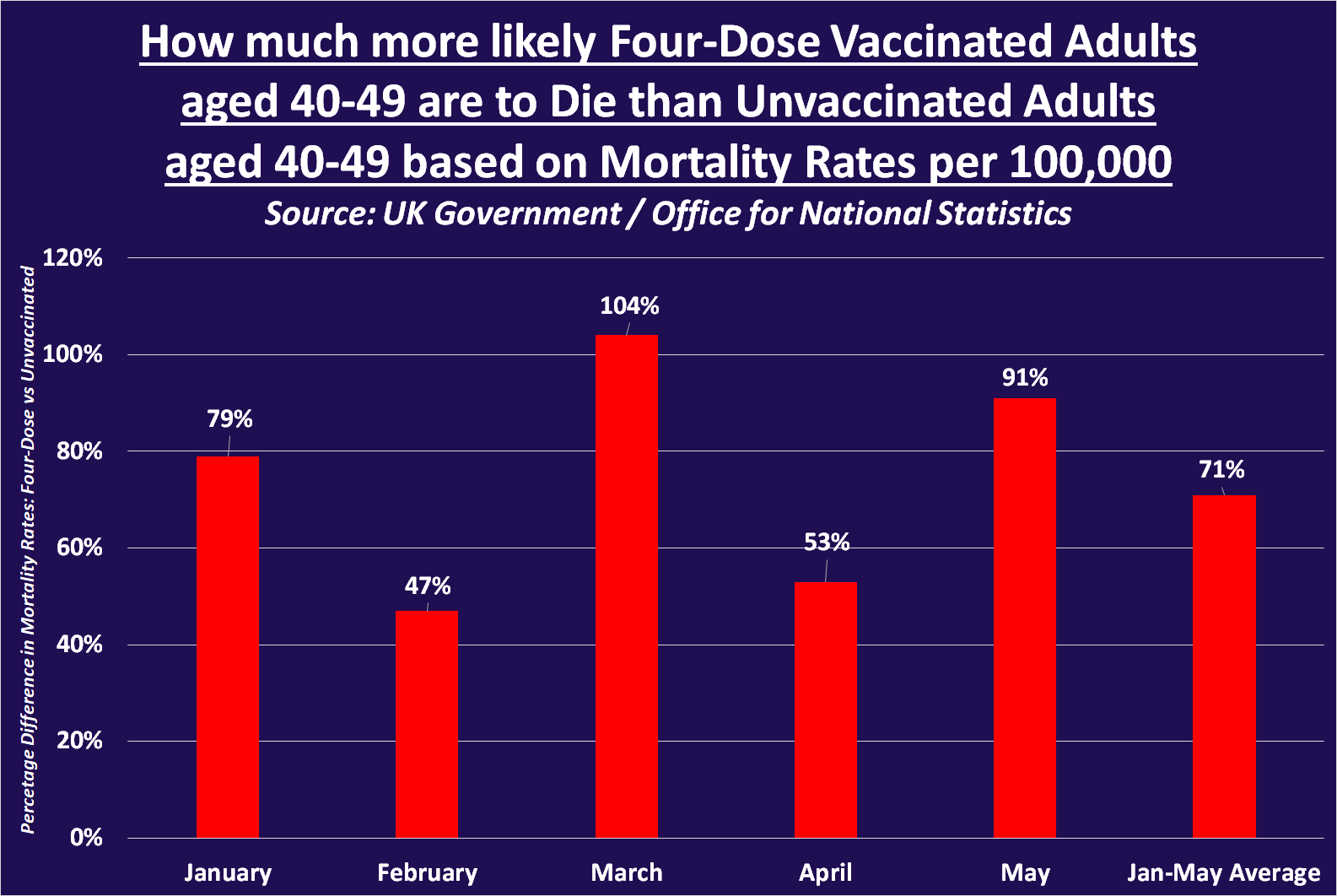 How much more likely 4 Dose Vaccinated 40-49 Die
Sources include:
|
|
Amish Paradise?The Amish have discovered the fountain of youthDoc Anarchy
Turns out, the Amish are healthy people. For some reason, this made national headlines, despite everyone with a functioning brain knowing this to be true.
The reason this story blew up is Steve Kirsch’s testimony to the Pennsylvania State Senate a few weeks back. In his testimony, he argued that the Amish were an excellent control group for the vaccinated vs unvaccinated populations. We’ll cover that later in the article.
That same testimony is what I have repeatedly found as the source of the claim that the Amish have zero autism, very little chronic disease, and very little cancer.
Let me start by saying, I haven’t been able to find the actual study. I searched for quite a while and the only thing I could find was this article by The Vigilant Fox . If you aren’t reading Fox’s work, you should. Amish HealthcareEveryone knows the Amish have some peculiar lifestyle traits. They follow strict rules as to what they can and cannot do, live far away from modern civilization, and have a tight-knit community.
Turns out, healthcare isn’t something they are forbidden from accepting. They are welcome, and in some cases encouraged, to seek medical care when needed.
The difference between the Amish and the average American is the Amish seek medical care when they actually need it. Before going to the doctor they seek guidance from elders and other experienced people in the community. They prefer to try natural remedies or home remedies before medicine. They give the body time to heal whatever ails it first.
If the body cannot heal itself and the natural remedies don’t work, they seek medical care from modern healthcare practitioners.
Compare this to the average American who goes to the hospital every time they stub their toe, blasted with X-rays, put on antibiotics, and then transferred to Hospice.
Yes, that’s an exaggeration. But the healthcare utilization rate in most of America is off the charts. Simply staying away from modern healthcare is a good way to extend your life. That means fewer unnecessary tests, a healthier environment, and less risk of medical error.
|
|
1 to 2 Cups of Coffee May Inhibit COVID Infection: StudyThat morning cup of Joe may do more than perk you up for the day; it could protect against infection from different COVID variants.By George Citroner
Your coffee habit may be doing double duty: jumpstarting your mornings and providing COVID-19 protection, according to a recent study.
New research reveals that coffee, enjoyed worldwide for its signature fragrance and flavor, may fend off illness by preventing SARS-CoV-2, the virus that causes COVID-19, from attaching to cells. Coffee—Regardless of Brew—Lowers RiskPrevious research shows that a diet rich in polyphenols (compounds in plants with antioxidant properties) may boost immune function and reduce the risk of severe COVID-19 symptoms. A recent study published in Cell & Bioscience went further and examined whether drinking coffee, which contains polyphenols, could also reduce the risk of COVID-19 infection.
Researchers conducted lab testing of human cells and a trial with 64 participants infected with a SARS-CoV-2 pseudo-virus. The lab tests found that coffee inhibited multiple SARS-CoV-2 variants by preventing viral binding to the ACE2 receptor on cells and reducing the activity of proteins linked to severe illness.
“Put simply, it kept the virus from getting the foothold needed to cause infection,” Dr. Jacob Teitelbaum, a board-certified internist, author, and director of the Practitioners Alliance Network, and not associated with the study, told The Epoch Times.
In the human trial, one to two cups of coffee daily inhibited infection across variants, including delta and omicron. The effect was consistent for various coffee types, including ground, instant, caffeinated, and decaffeinated.
The authors suggested coffee could be an effective dietary strategy to prevent COVID-19. Coffee Tied to Reduced Risk in Prior Large StudyThe new study had human participants but adds to evidence from a much larger 2021 Northwestern University study. Researchers analyzed data from the UK Biobank, a large-scale biomedical database, entailing the dietary behaviors of almost 38,000 people between 2006 and 2010 to determine if their past diet impacted their COVID-19 infection risk in 2020.
They found that drinking at least one cup of coffee per day was linked to a 10 percent lower risk of COVID-19 infection compared to lower daily coffee consumption.
Additionally, the study found that eating vegetables was also associated with lower infection risk; about ¾ cup of non-potato vegetables daily appeared protective. However, researchers also discovered that less than half a daily serving of processed meat (but not red meat) increased the risk of COVID infection. Coffee’s Other Health BenefitsThe following are three significant health benefits already associated with drinking coffee:
“So this is more of the data that supports enjoying your coffee,” Dr. Teitelbaum said. Easy but Powerful Ways to Boost ImmunityThough coffee may offer protection, there are more powerful ways to prevent COVID-19, according to Dr. Teitelbaum.
In households where somebody gets the disease, only 1 in 6 other members will also catch it on average, though that rate was 2 in 5 for the higher for the more infectious omicron variant. Dr. Teitelbaum said low transmission rates in households show that immunity is far more important than viral exposure. In other words, it’s not the disease that matters so much as the health of the person exposed to it.
Three effective ways to easily boost the immune system include the following:
1. Take VitaminsDeficiencies in immunity-influencing vitamins A, C, D, and E and zinc can increase susceptibility to infections. Dr. Teitelbaum recommends a multivitamin plus elderberry and zinc supplements. “These dramatically improved immunity,” he said.
2. Stay Hydrated“The part of the immune system that initially fights COVID is like our Navy,” Dr. Teitelbaum said. “It works poorly in dry dock.”<
Research shows dehydration can reduce disease-fighting capability. But don’t reach for sugar-sweetened drinks. “The amount of sugar in one can of soda or orange juice can decrease immune function by 30 percent for three hours,” Dr. Teitelbaum said.
3. Get Enough SleepInadequate sleep substantially reduces our ability to fight illness. The optimal sleep duration is seven to eight hours nightly for most adults, nine to 10 for teenagers, and 10 or more for school-aged children.
While offering potential benefits, excessive coffee intake (over four cups a day) can cause adverse effects like insomnia, rapid heartbeat, and tremors. It’s important to moderate coffee consumption and avoid adding excessive sugar, as this increases obesity and diabetes risks.
George Citroner
|
|
Florida Doctor Reinstated After Losing Board Certification for Criticizing COVID-19 VaccinesWith money raised for legal fees, physician plans to help medical students under pressure to submit to ‘woke’ ideology Dr. John Littell speaks at a press conferencein Kissimmee, Fla., on Oct. 13, 2022, about people he says were injured by COVID-19 vaccines and government-recommended treatment protocols for the disease. (Nanette Holt/The Epoch Times) By Natasha Holt
A Florida physician known for being outspoken about COVID-related topics has regained his board certification that was stripped because he publicly criticized COVID vaccines.
Now, Dr. John Littell is moving forward from the experience with plans to help future physicians defend themselves when disciplined for voicing viewpoints that are not in the majority, he told The Epoch Times.
Dr. Littell, a longtime family physician in Ocala and a medical school professor, began posting videos sharing his thoughts about COVID-19 testing, treatments, and vaccines early in the pandemic. He was frustrated to find his content often was pulled down from his YouTube channel.
But he fought against what he saw as censorship by moving the content to other platforms, such as Rumble, he said. Then, in January 2022 and again five months later, he received warning letters from the American Board of Family Medicine (ABFM), the organization that issued his certification for his medical specialty.
The letter stated that his videos on YouTube and Rumble spread “medical misinformation” and could put his board certification in jeopardy, he said.
The ABFM declined to comment on the matter because the board’s “policy indicates we are unable to comment about professionalism cases,” an unidentified spokesperson said in an email to The Epoch Times.
The ABFM is the third largest of the 24 boards of the American Board of Medical Specialties. More than 100,000 family medicine doctors are certified by the board, according to its website.  Protesters concerned about treatment of people who died while being treated for COVID-19 stand outside a board meeting at Sarasota Memorial Hospital in Sarasota, Fla., on Feb. 21, 2023. (Courtesy of Tanya Parus) To keep their certification, physicians must uphold the board’s ethical standards and “guidelines for professionalism, licensure, and personal conduct,” the website states.
In letters from the board, Dr. Littell was told his public statements violated those guidelines. Dr. Littell responded to the letters and continued to speak publicly and post videos about the subjects, he said.
Months later, when he didn’t hear back, he said he thought the threat was gone. “I was very happily under the radar,” he said.
Exposing the FDA’s Orwellian Lie About Ivermectin | CLIP | Facts MatterOutrage Over Ivermectin
That changed after he was escorted out of a Sarasota Memorial Hospital board meeting in February for approaching a board member behind the dais. He wanted to thank the board member, he said, for letting him speak at the meeting. He didn’t realize that move would be seen as inappropriate, he said.
Though he’s cared for many patients in hospitals, he’d never attended a hospital board meeting, let alone a contentious one, he said.
That day, medical freedom activists filled the boardroom to speak against the public hospital’s policies during the COVID-19 pandemic. Many were angry their loved ones were denied the opportunity to try ivermectin, an antiparasitic for humans and animals widely used by some in treating COVID-19, and other treatments.
Dr. Littell spoke cordially to board members from the podium, an Epoch Times reporter confirmed. He told board members how treating patients with ivermectin had been his key to success in helping them recover. And he praised hospital personnel for their work during the pandemic.
Shortly after that, security guards escorted him outside.  Retired Army Gen. Michael Flynn, who served briefly as national security advisor for former President Donald Trump, attended a board meeting of Sarasota Memorial Hospital in Sarasota, Fla., on Feb. 21, 2023 (Chris Nelson for The Epoch Times) A video of Dr. Littell’s removal from the meeting by security guards was posted to social media and received millions of views and media coverage. And that thrust him back in the spotlight as a doctor vocal about COVID-19 policies. He questioned whether someone else would have been removed for the same reason.
Many doctors have faced consequences for questioning the efficacy and safety of COVID-19 vaccines and for advocating for the use of medicines such as ivermectin in the treatment of the disease.
The U.S. Food and Drug Administration (FDA) wrote in one social media post about ivermectin: “You are not a horse. You are not a cow. Seriously, y’all. Stop it.” It linked to a page entitled “Why You Should Not Use Ivermectin to Treat or Prevent COVID-19.”
Three doctors sued the FDA over the statements, saying it had no power to tell doctors which drugs to prescribe. On Sept. 1, a federal court ruled that the agency likely overstepped its authority when it told Americans to “stop” using ivermectin against COVID-19. The FDA can inform, but has “no authority” to recommend consumers “stop” taking medicine, U.S. Circuit Judge Don Willett wrote in the ruling. Accused of ‘Spreading False’ InformationThe month after Dr. Littell spoke in Sarasota, the board sent a letter saying he’d been de-certified for “spreading false, inaccurate, and misleading materials about COVID-19, COVID-19 vaccination, and treatment and mitigation of the virus,” The Epoch Times confirmed.
A letter reviewed by The Epoch Times stated that if Dr. Littell appealed the decision within 20 days, he would continue to be represented by the board, pending a review of his case by the professionalism committee of the ABFM board of directors.
The reason for the decision to review his record was because of his past suggestions the COVID-19 vaccine was a product of genetic engineering, causing deaths in children and causing the rise of the Delta variant, the letter indicated. It also referenced “false” statements made by Drs. Ryan Cole and Robert Malone, who spoke at a medical freedom conference Dr. Littell organized in October 2022.
In the letter, the board also criticized Dr. Littell for “offering to provide medical exemptions from vaccination” to patients across the country and “publicly comparing the U.S. public health system’s response to the COVID-19 pandemic to Nazi Germany.”
After receiving the troubling letter, Dr. Littell sought the help of attorney Jeff Childers, a business attorney in Gainesville, Florida. Since the COVID-19 lockdowns began, Mr. Childers has become active in lawsuits around the country related to medical freedom. He authors a daily blog called Coffee and Covid, which started by chronicling COVID-19 issues and now tracks other social and political issues, as well.
Mr. Childers crafted a 64-page appeal to the board, dissecting every accusation made against Dr. Littell, an Epoch Times reporter confirmed. And as word of the threat to Dr. Littell’s board certification spread—a move that would prevent him from practicing medicine—medical freedom activists rose up to take his side.  Florida attorney Jeff Childers. (Amber Bertrand for The Epoch Times) A GiveSendGo.com campaign was started to collect donations to fund his legal fees. More than 6,400 people donated almost $255,000. And more than 1,900 pledged to pray for Dr. Littell.
The Global Covid Summit, an international group of doctors focused on medical freedom in COVID-19 treatment, sent a letter signed by 169 doctors to the ABFM in support of Dr. Littell. In the letter, they argued that the board was false in every accusation made against Dr. Littell.
Florida Surgeon General Joseph Ladapo also voiced support for Dr. Littell. “What they’re doing is being a bully,” he said in an interview with The Floridian. “It’s not going to age well. “I read the letter from the Board, and it’s dripping with political animosity.” Both Rep. Pete Sessions (R-Texas) and Dr. Littell’s congresswoman, Rep. Kat Cammack (R-Fla.) sent letters in his defense to the board, Dr. Littell said.
“I’ve got to believe it’s not in the dozens, but probably in the hundreds of people who called and sent letters to the American Board of Family Medicine,” Dr. Littell said. “I never asked them to, but that is what was happening.”
In July, Dr. Littell received word that the board had reviewed his case and retroactively de-certified him for three months, from March 16 to June 16. He never stopped seeing patients.
“It’s like a slap on the wrist so they’d feel good about it, but wouldn’t, presumably, have to face any legal action,” he said. His attorney agreed. “They did it in a very face-saving way,” Mr. Childers said. But ultimately, he’s pleased with the decision. “We were really surprised and gratified that we were able to achieve that result,” Mr. Childers said. Dr. Littell credits it to being “a God thing” that he was able to keep caring for patients and face a decertification period only retroactively.
“If they had said I was decertified, I would not have been able to do what I was doing. I mean, especially with the hospital care patients. I could have gotten into big trouble.”
He still may face consequences for having the blemish on his record, he said. He’ll have to report it to the hospitals at which he works and explain what happened, he said.
“Every time I go up for privileges with a hospital or any other institution, they’re going to say, ‘Well, has your license ever been suspended or revoked, and has your board certification ever been revoked?’ So, it’s still an issue. It’s not like you can just forget about it.”
He’s been advised by some other doctors, such as cardiologist Peter McCullough, to pursue legal action for the disciplinary measure they feel was wrong, he said. Continuing to Speak OutDr. Littell continues to speak out about the same topics. So he suspects he’ll face retribution again, he said. “The way I read the letter, it’s sort of like a warning,” Dr. Littell said. The board, he said, seemed to be sending the warning, “If you act up again, we know it’s a privilege to have this board certification, and it can be removed at any time.” And the next time, the punishment is likely to escalate. “The implication is that if it happens again, it’s going to be more than just three months,” Mr. Childers said. Around the country, a slew of doctors had board certifications removed and licensure threatened for sharing their COVID-related opinions.
“Most people would probably be surprised to find out there’s a lot of this going on, now that the pandemic is over,” Mr. Childers said. “From what I’ve heard, there’s probably more challenges to doctor licensing right now than at any other time.”
But because most doctors aren’t vocal about receiving discipline, it’s hard to know exactly how often it’s occurring, he said. Doctors who have been active on social media seem to be targeted more often by medical authorities, he said.  Dr. Peter McCullough speaks in the Mississippi capitol building on COVID-19 vaccine adverse events. (Courtesy of Charlotte Stringer Photography) Doctors who were not actively posting their thoughts about COVID-19 on social media “should feel very confident that if they follow a similar approach to what Dr. Littell did, they could hope for a good result at this point,” he said.
Obtaining good legal advice is key, he said. It also helps to spread the word. “All too often doctors either ignore these kinds of letters until it’s too late because they’re embarrassed, or they try to handle it on their own,” he said.
“It’s important that people know when this happens. And if they’ll let folks know, they’ll find that they get a lot of support.” Dr. Littell has no plans to keep quiet about what he feels went wrong during the COVID-19 pandemic “I’m not letting up,” he said. He’s organizing his third annual medical freedom summit in November called “Food, Family & Medical Freedom” in Ocala, Florida at the World Equestrian Center. Helping Future DoctorsHe intends to use the remaining money donated to his legal fund to help others respond to similar licensure problems, especially threats faced by medical students, he said.
He’s trying “to come up with a legal, legislative, and public relations strategy that helps future physicians,” he said. When they see practicing doctors disciplined and “raked over the coals” for speaking out about medical freedom issues, it deters good people from pursuing a degree in medicine, he said.
“I would like the medical freedom fighters, as I’m calling them, to create a sanctuary for pre-med, especially, and medical school students.”
“Early on, even in the colleges, they weed out the physicians who dare to question the narrative or challenge it,” he said, of those who insist that doctors decrees made by federal health agencies.
But asking questions and challenging prevailing thought is important to the goal of continually improving medical treatments, he said.
“And that intellectual curiosity is what we’re so desperately lacking now in medicine, and in most professions.” He also envisions the network expanding to help connect like-minded educators in colleges, universities, and medical schools to share their ideas without fear of being in opposition to “woke” ideology, he said.
He hopes to see that network push back against “lockstep mentality” and help students who are suffering because of it. Medical students taught by Dr. Littell often tell him how difficult it is to be entering the field of medicine at this time, he said.
One student told him that his second-year class was forced to be vaccinated for COVID-19, he said. Classmates were told by their university they’d be “thrown out” of medical school in two weeks if they didn’t comply, Dr. Littell said.  Medical freedom activists upset about COVID-19 vaccines and other issues gather to voice concerns to lawmakers on the first day of the Florida Legislature’s annual regular session at the Capitol in Tallahassee on March 7, 2023. (Courtesy of Justin Harvey) The student told him that, although more than half the class didn’t want the vaccine, they felt they had no other option, Dr. Littell said. Weeks later, the mandate was lifted. But it was too late—many students already had submitted to getting the shot they didn’t want.
“It’s like they [university officials] were playing games,” he said. “And the students didn’t know any better. “They just don’t have enough support,” Dr. Littell lamented. “They want to say things, but they’re afraid they’re going to get disciplined if they speak out.”
He sees bringing people together to unite in their pushback against prevailing opinions as a revolutionary concept. “It’s really no different than what our Founding Fathers did,” Dr. Littell said. “They realized that they were victims of repression. But there also were people comfortable with the status quo. That’s what is in our medical schools right now and is what we all need to fight against.
“People should be allowed to question and use their God-given intellect, and not be censored or disciplined for doing so.” Zachary Stieber contributed to this report. Natasha Holt |
|
People Rarely Transmit COVID-19 Before Experiencing Symptoms: Lancet Studyby Tyler Durden, 06September2023 – https://www.zerohedge.com/medical/people-rarely-transmit-covid-19-experiencing-symptoms-lancet-study
Authored by Tom Ozimek via The Epoch Times (emphasis ours),
In a blow to the COVID-19 “silent spreader” narrative that has been used to push for universal masking, including controversially among schoolchildren, a recent study published in The Lancet suggests that people who are non-symptomatic rarely have the ability to infect others.
Silent transmission is the idea that those who are infected with COVID-19 but show no symptoms can still spread the virus to other people.
While all relevant studies show that presymptomatic and asymptomatic “silent spreaders” account for some proportion of infections in other people, the degree of silent transmission is less clear.
A number of early studies—in some cases affected by limitations that may have led to their proportion of presymptomatic transmission to be “artifactually inflated”—suggested that silent transmission accounted for around half of secondary infections, or even more.
The early studies led public health authorities to argue that everyone should wear a mask at all times when out in public or crowded places. This, in turn, helped drive draconian universal masking policies, including in schools, in a bid to reduce the spread of COVID-19.
For instance, Dr. Anthony Fauci, former director of the National Institute of Allergy and Infectious Diseases (NIAID), initially discouraged universal mask-wearing early in the pandemic but later did a U-turn.
Initially, “we didn’t realize the extent of asymptotic spread,” Dr. Fauci said in July 2020, adding that later, “we fully realized that there are a lot of people who are asymptomatic who are spreading infection.”
“So it became clear that we absolutely should be wearing masks consistently,” Dr. Fauci said at the time. But new research calls into question the significance of the threat of silent transmission, which comes as COVID-19 cases are on the rise in America, driving what some are calling a renewed pandemic “hysteria” and calls for a fresh round of restrictions, including mask mandates. ‘Very Few Emissions’ Before Symptom OnsetThe new study, published in the August issue of The Lancet’s Microbe journal, shows that people who are sick with COVID-19 but don’t show any symptoms have a limited ability to spread the virus to other people.
Participants in the British study, which was carried out by researchers at Imperial College London, were unvaccinated healthy adults aged 18-30 who were intentionally infected with COVID-19.
The subjects were monitored under controlled circumstances while self-reporting symptoms three times per day, and researchers collected nose and throat swabs from them daily, checking for the presence of the virus.
The researchers also tested the inside of masks worn by the participants, checked their hands, and examined the air and surfaces of rooms that the subjects were kept in for a minimum of 14 days. Ultimately, the researchers found that less than 10 percent of the viral emissions from infected participants took place before the first symptoms emerged.
“Very few emissions occurred before the first reported symptom (7%) and hardly any before the first positive lateral flow antigen test (2%),” the authors of the study wrote.
The new study—which takes the form of a rigorous, controlled “challenge study” rather than the earlier modeling studies that relied on subjective inputs and assumptions of researchers—contradicts earlier research that set the tone for much of the prevailing narrative. That early research appears to have inflated the perceived threat of presymptomatic spread.
The latest study, suggesting that silent transmission is far less significant, comes amid a growing drumbeat of alarm as COVID-19 cases, hospitalizations, and deaths are on the rise—along with calls in some circles for renewed restrictions.
By contrast, many are calling for cool heads to prevail—or are urging civil disobedience if lockdowns or other mandates are reimposed. ‘Artifactually Inflated’?Some early studies, such as one published in August 2020 called “Temporal Dynamics In Viral Shedding and Transmissibility of COVID-19,” suggested that people who were presymptomatic or asymptomatic accounted for a large proportion of secondary infections.
This particular study estimated that 44 percent of secondary cases were infected during the presymptomatic stage, while concluding that “disease control measures should be adjusted to account for probably substantial presymptomatic transmission.”
The authors of the study admitted that it had several limitations, however, including potential “recall bias” that may have tended towards a delay in recognizing first symptoms.
“The incubation period would have been overestimated, and thus the proportion of presymptomatic transmission artifactually inflated,” meaning that the study may have exaggerated the proportion of people who spread the virus before showing symptoms, they said.
Another study from July 2020 called “The Implications of Silent Transmission for the Control of COVID-19 Outbreaks” went even further, suggesting that people were most infectious during the presymptomatic phase and concluding that silent transmission was the “primary driver of COVID-19 outbreaks and underscore the need for mitigation strategies, such as contact tracing, that detect and isolate infectious individuals prior to the onset of symptoms.”
That study relied on a range of assumptions and models, with different presymptomatic, asymptomatic, and symptomatic transmission rates calculated based on a complex mathematical model from another study.
Findings from earlier studies like the ones cited above led public health officials to argue that silent spreaders were a big factor in COVID-19 transmission and so to recommend that everyone should mask up. |
|
Israeli Health Ministry ‘lost’ 82% of reports on COVID vaccine side effectsAuthorities forced vaccinations on Israeli population, leading to increase in adverse events
Posted by Yudi Sherman
Israel’s Health Ministry failed to review 82% of reports on side effects from Pfizer’s COVID-19 vaccine, according to a recent official report.
Comptroller: Ministry recorded only 18% of reportsState Comptroller Matanyahu Englman revealed last month that the Israeli Health Ministry received 345,200 reports of adverse events following administration of the Pfizer injection. Only 18% of those reports were recorded in the ministry’s database. The other 82% were “lost” due to “technical errors,” Times of Israel reported.
“The Health Ministry also failed to process an additional 33,000 reports filed by the public regarding side effects due to limited ability to analyze reports filed anonymously,” continued the report. “Adding to that, a lack of manpower in the ministry’s Department of Epidemiology meant that reports that contained identifying details were also unable to be reviewed and investigated.”
Ministry failed to investigate serious side effects in timely mannerThe 18% of reports that were reviewed by the Health Ministry mostly consisted of mild side effects such as pain at the injection site or low fever.
There were also reports about more serious side effects that made it to the review stage and were checked by ministry officials. These included approximately 200 reports about changes in vaccinated women’s menstrual cycles following the shots. However, Comptroller Englman found that the ministry did not investigate these reports in a timely manner.
The ministry also reviewed only about 275 reports about myocarditis and pericarditis following the injections. Most of the patients in those cases ended up being hospitalized.
Rather than criticizing public health officials for failing to investigate the great majority of vaccine injuries, however, Comptroller Englman’s report chastised the Health Ministry for not doing enough to ensure public trust in the mRNA injections. He specifically reprimanded government officials for not acting sufficiently to combat “anti-vaccination propaganda” and for not having a strategy in place to fight “false information” about the vaccine.
Israel: A ‘lab for Pfizer’During the pandemic, Israeli officials repeatedly told the public that the vaccine’s side effects were mild and that serious adverse events were “rare.” These claims were used to justify forced vaccinations, where Israelis who refused the shots were barred from schools, restaurants, pools, events, driving tests, and public areas.
Officials proudly declared Israel as a “lab for Pfizer,” being the first country to experiment with the COVID-19 vaccines. Israel’s rollout provided the data for other countries to then roll out their own vaccination campaigns.
Israel was also among the first to implement harsh vaccine mandates for nearly all age groups, adding to a mask mandate which police violently enforced. These were accompanied by harsh rhetoric from officials, who blamed deaths and lockdowns on the unvaccinated. Then-Prime Minister Naftali Bennett proposed increasing health insurance premiums for those who refused the shots, and tried to implement a bracelet system to publicly identify the unvaccinated.
Forced vaccinations for young and healthy Israelis despite no COVID deathsAll this was justified by daily reports from the Health Ministry showing thousands of COVID-related deaths among all adult age groups.
But in response to a Freedom of Information (FOI) request from attorney Oren Shabi, Israel’s Health Ministry admitted last year it had no record of deaths among those 18-49 with no comorbidities.
“Among COVID-19 deaths on which epidemiological research was conducted and comorbidities were disclosed, there are 0 recorded deaths among ages 18-49 with no comorbidities,” said the ministry.
Many Israelis within that population were nevertheless forced to take the injections, which were then tied to a sudden increase in cardiac events.
A 25% increase in cardiac events among young and healthy IsraelisA Massachusetts Institute of Technology (MIT) study in 2022 of young, healthy Israelis found that with the advent of the COVID-19 vaccine those Israelis saw a 25% increase in cardiovascular events.
MIT researchers studied emergency calls in Israel over a two-and-a-half-year period spanning 2019-2021. Specifically, they looked at emergency calls reporting either cardiac arrests [CA] or acute coronary syndrome [ACS] in the 16-39 age group.
The study also aimed to determine whether the uptick in cardiovascular events was associated with COVID-19 or the COVID-19 vaccine. The findings showed that for the period of January–May 2021 there was a 25% increase in emergency cardiovascular events compared with the same period in 2019 and 2020, and was entirely associated with the COVID-19 shot.
Israel’s Health Ministry vehemently denied there was any increase in cardiac arrests, though. In the same letter to Shabi, however, the ministry revealed that it stopped recording cardiac arrest data in 2021.
|
|
COVID-19 Vaccines Revealed as ‘Neither Safe, Nor Effective’: WatchdogThe vaccines were hastily approved through an ‘interim order’ that enabled pharma companies to bypass approved procedures.By Naveen Athrappully
COVID-19 vaccines were authorized in Canada during 2020 and 2021 without being subjected to the country’s safety tests as required under established drug regulations, an accountability watchdog revealed.
An investigation into COVID-19 vaccines found that they were “neither safe nor effective,” according to the nonprofit organization National Citizens Inquiry (NCI). The organization published a report on Sept. 14 detailing the flawed mechanism through which the vaccines were granted “approval” in Canada.
“It is important to understand that the COVID-19 vaccines were never approved under the traditional approval process for drugs in Canada,” the report states (pdf). Instead, Health Canada, the federal agency responsible for national health policy, approved the vaccines through an alternative authorization process—an interim order.
“Under the alternative authorization process, the necessity to establish the safety and efficacy of COVID-19 vaccines through an objective manner appears to have been set aside,” the report states.
Canada’s Food and Drug Regulations require that a drug can only be approved in the country after its safety and effectiveness are demonstrated to the minister of health. Then, the minister considers whether the benefits outweigh the risks, following which, approval is granted.
Instead of following regulations, the minister of health sanctioned an interim order on Sept. 16, 2021, which exempted all COVID-19 vaccines from normal review and approval. This provision usually allows the minister to override normal regulations in situations of “significant risk” to health, safety, or the environment.
In Canada, four COVID-19 vaccines were authorized by the health agency under an interim order—Pfizer-BioNTech, Moderna, Janssen, and AstraZeneca.
The report notes that under the order, vaccines were authorized under a “subjective test.” In this situation, authorization is granted by simply proving that the benefits of vaccination outweigh the risks.
“This cannot be an appropriate standard for approving a drug that the Government intends to administer to the entire population. It is difficult to conceive of a less-scientific test for drug authorization than that found in the Interim Order,” the report states.  A child receives a dose of the Pfizer-BioNTech COVID-19 vaccine at the Fairfax County Government Center in Annandale, Va., on Nov. 4, 2021. (Chip Somodevilla/Getty Images) Moreover, the order made sure that the vaccine authorizations couldn’t be revoked even under evidence that they were unsafe and ineffective. Once an interim order is issued, the typical Food and Drug Regulations don’t apply.
The order thus exempted manufacturers from having to effectively demonstrate “objective evidence of safety and effectiveness” of their COVID-19 vaccines.
“The result was that while chief medical officers across the country repeatedly assured Canadians that the COVID-19 vaccines were ‘safe and effective’—the general Canadian population had no understanding that their authorization process had not required objective proof of safety nor efficacy,” the report states. ‘Not Safe for Human Use’The NCI report was supported by cardiologist Dr. Peter A. McCullough. “Excellent work @Inquiry_Canada with exhaustive testimony and evidence review. Conclusion: all COVID-19 vaccines unsafe for human use and must be removed from the Canadian market immediately to protect the public,” he wrote in a Sept. 16 post on X. Dr. Peter McCullough, a cardiologist, speaks at the Conservative Political Action Conference at the Hilton Anatole in Dallas on Aug. 5, 2022. (Bobby Sanchez/The Epoch Times) Dr. McCullough recently asked European lawmakers to take COVID-19 vaccines off the market due to concerns about illnesses such as heart inflammation, blood clots, and neurological diseases.
“COVID-19 vaccines and all of their progeny and future boosters are not safe for human use. I implore you, as a governing body, European Medicines Agency, to apply all pressure and due urgency to remove the COVID-19 vaccines from market,” Dr. McCullough said in Sept. 13 testimony to the European Parliament.
The NCI report comes as the U.S. Food and Drug Administration (FDA) approved new COVID vaccines on Sept. 11 for children as young as 6 months old.
“Vaccination remains critical to public health and continued protection against serious consequences of COVID-19, including hospitalization and death,” Dr. Peter Marks, a top FDA official, said in a statement.
However, many experts have questioned the push for new vaccines. Earlier this month, Florida Surgeon General Dr. Joseph Ladapo criticized the updated vaccines.
“We all know there’s a new vaccine that’s coming around the corner, [a] new mRNA COVID-19 vaccine. And there’s essentially no evidence for it,” he said during a press conference.
“There’s been no clinical trial done in human beings showing that it benefits people, there’s been no clinical trial showing that it is a safe product for people. And not only that, but then there are a lot of red flags.”
Dr. Ladapo said that mRNA COVID-19 vaccines have “caused cardiac injury in many people.” Not Actually ‘Interim’Canada’s interim order for COVID-19 vaccines “has become permanent,” according to the NCI report. An interim order typically only lasts for one year. In March 2022, the order was replaced with permanent regulations, which codified the “subjective authorization” of the vaccine.
“Thus, under the permanent test, Health Canada no longer has to be swayed by urgency, but simply by the public health need related to COVID-19. In this way, it seems that so long as COVID-19 is a circulating virus, Health Canada must authorize any vaccine for which there is an argument to support the conclusion that its benefits outweigh its risks,” the report states.
“In effect, we fear that there will never be a need for COVID-19 vaccine manufacturers to prove [the] safety or efficacy of their products.”
NCI also alleged there was a “conflict of interests” while approving the COVID-19 vaccines, with the government being involved.
The Epoch Times reached out to Health Canada for comment but didn’t receive a reply by press time. Political Interests, Letter to TrudeauCanada usually doesn’t allow drugs to be imported into the country unless approved by Health Canada. However, the interim order allowed the unapproved COVID-19 vaccines to be imported “as long as the Canadian Government was the purchaser,” according to the report.
This pre-purchasing and distribution of COVID-19 vaccines were done to make sure that they were available for dissemination as soon as they were authorized.
“This created a tremendous conflict of interest,” the report states. “Once the vaccines were purchased, imported and ready for distribution, the Government of Canada would have suffered significant political blowback if it was unable to authorize them. Thus, it needed to authorize the COVID-19 vaccines, and it needed to do it quickly.
“The Government of Canada ordered the vaccines, imported them, created new regulations to authorize them, and then took significant measures to convince and coerce every Canadian to take multiple doses. The political stakes were high, and the federal government had every motivation to get the vaccines authorized, regardless of their actual efficacy or safety.”
On Sept. 14, the NCI sent a letter (pdf) to Canadian Prime Minister Justin Trudeau highlighting the issue of COVID-19 vaccine approval.
“Canadians are relying on representations as to the safety and effectiveness of COVID-19 vaccines,” which Health Canada has never determined, the letter said. “Some might draw the conclusion that the misrepresentation to Canadians of proven safety is intentional, made while knowing it to be false and intending it to be relied upon.
“As a matter of common sense, the objective falsity of the ‘proven safe’ claim brings into question the basis for informed consent to the administration of the injections, creating potentially enormous liabilities.”
In the current context, the organization pointed out that the population immunity has increased along with the latest variants being “milder.”
“In the face of your government’s reported intention to promote booster injections in coming months, the urgency now lies in telling the truth to Canadians and taking corrective action,” the letter reads.
The NCI asked the prime minister to withdraw COVID-19 vaccines “until the normal rigorous evaluation can be completed” and to reinstate the traditional objective test for safety.
Naveen Athrappully
|
|
Pfizer-Funded Study Shows Poor Effectiveness for COVID-19 Vaccine in Young ChildrenThree doses of the Pfizer vaccine provided little protection against emergency room visits, urgent care encounters, or outpatient visits.By Zachary Stieber
A new study funded by Pfizer found the company’s COVID-19 vaccine did not perform well in children under 5.
Children aged 6 months to 4 years are supposed to receive three shots of the Pfizer-BioNTech vaccine. The number was increased from two when early testing showed little effectiveness.
Three doses of the Pfizer vaccine provided little protection against emergency room visits, urgent care encounters, or outpatient visits, according to the new study.
Researchers with and funded by Pfizer analyzed records from Kaiser Permanente Southern California. They included patients who tested for COVID-19 at an emergency department, urgent care, or outpatient setting along with being diagnosed with acute respiratory infection. The date range was July 23, 2022 through May 19, 2023.
Positive cases were those with a positive test result. Controls tested negative and had no evidence of prior infection in the past 90 days. Children were only counted as vaccinated if they received a second or third shot two or more weeks before being exposed to COVID-19. Children were excluded if they only received one dose, received any doses from a different company, or did not follow the recommended dosing schedule.
After adjusting for factors such as age and sex, researchers estimated just 12 percent effectiveness against medically-attended encounters for children who completed the three-dose primary series.
Confidence intervals crossed well over one, indicating that the effectiveness might actually be worse or even negative.
The effectiveness was estimated to be higher, or 44 percent, for children who received two doses of the regimen
Researchers speculated that the difference stemmed from more immune-evasive virus variants becoming dominant in the United States by the time children received a third dose.
“Updated vaccines will likely be needed to maintain protection against contemporary Omicron strains in young children,” they wrote.
The study was published by the Journal of the American Medical Association.
Sara Tartof, the study’s corresponding author and an employee of Kaiser Permanente Southern California, did not answer questions, including why researchers included those with two doses but not those with one dose.
Pfizer did not return a request for comment. A child receives a dose of the Pfizer-BioNTech COVID-19 vaccine at the Fairfax County Government Center in Annandale, Va., on Nov. 4, 2021. (Chip Somodevilla/Getty Images) Key Problems
FDA Detects Serious Safety Signal for Covid Vaccine Among Kids
Among the key problems with the research were only including children who were diagnosed with acute respiratory infection (ARI), Dr. Robert Malone, who was not involved in the research, said.
That “may predispose to young children that lack a primary care physician/pediatrician,” Dr. Malone, who helped invent the mRNA technology Pfizer’s vaccine utilizes, told The Epoch Times via email.
“Likewise, the control group of non-vaccinated with ARI will also have selection bias. These intrinsic study biases make the relevance of the measured outcome to the general population quite problematic.”
Another issue is using positive results on polymerase chain reaction testing as the metric for having COVID-19, given the false positives the testing brings, Dr. Malone said. Some patients who tested positive may actually have another virus, such as influenza, he said. Need a TrialPfizer’s vaccine was authorized for children despite unreliable efficacy estimates against infection, and no efficacy estimates against severe disease.
The newly reported results are based on a test-negative design, which is inappropriate for measuring effectiveness, said Dr. Jay Bhattacharya, professor of health policy at Stanford University.
“The design starts with children who are already seeing a doctor and then makes strong and unsupportable statistical assumptions to derive the probability of seeing a doctor for vaccinated and unvaccinated children,” Dr. Bhattacharya, who was not involved in the research, told The Epoch Times via email.
“What is needed to answer this question without bias is a randomized control trial. I am shocked that the FDA has not asked Pfizer and Moderna to conduct such a study,” he added.
The U.S. Food and Drug Administration (FDA) cleared Pfizer’s shot on the basis of immunobridging, or comparing antibody levels in children after vaccination with levels in adults after vaccination.
Antibodies are believed to protect people against COVID-19.
The authorization has been the subject of protests, including a complaint that said the FDA violated its own standards with the clearance.
The FDA this month cleared new vaccines from Pfizer and Moderna for children. The only trial data was from 50 people aged 12 or older who received Moderna’s shot. The U.S. Centers for Disease Control and Prevention (CDC) recommended the shots to all people aged 6 months and older. CDC DataCDC data presented on Sept. 12 showed that both the Pfizer and Moderna vaccines failed to provide much protection to young children.
One dose of Pfizer’s vaccine provided just 8 percent protection against emergency room and urgent care visits beyond 13 days, while two doses provided a peak of 44 percent protection, according to the data (pdf).
A third dose provided 71 percent protection between 14 and 59 days, but the shielding plunged to 16 percent after two months.
A two-shot primary series of Moderna’s shot initially provided 46 percent protection. That shielding dropped even lower, to 24 percent, beyond 60 days.
The World Health Organization considers 50 percent as adequate effectiveness for vaccines.
A single dose of a bivalent shot, introduced in the fall of 2022, boosted protection to 61 percent, but no estimates were available over time and the estimate was based on just eight vaccinated patients who tested positive.
“This imprecision indicates that the actual [effectiveness] could be substantially different,” the CDC said.
Zachary Stieber
|
|
Undeniable Severe Injuries After HPV VaccinationThe HPV Vaccine: A Golden Shield or a Double-Edged Sword? (Part 2)A collection of documented evidence is presented for serious injuries associated with Gardasil. Their existence is undeniable. By Yuhong Dong
Dear Readers, I would like to sincerely apologize for not being able to continue this series for about two months due to being called for another urgent and important assignment. Now I am back to this series. Dr. Yuhong Dong In this series, “The HPV Vaccine: A Double-Edged Sword?” we will provide a collection of documented evidence of death and serious injuries associated with Gardasil. Their existence is undeniable. We will also analyze the potential mechanisms for serious adverse events and disclose important facts about the vaccine. We will conclude with a discussion about the underlying root causes for the phenomena behind the HPV vaccines and will provide recommendations for key stakeholders.
Previously, in Part 1 of this series, we presented documented evidence of death cases in young girls or boys with undeniable association with Gardasil.
In Part 2, we present documented evidence of non-fatal but severe injuries in children who were healthy and lost their ability to live normally after receiving the human papillomavirus (HPV) vaccine—believed to be one of the most effective vaccines developed to date. Gardasil was launched in the United States, Germany, and Denmark in 2006 and in Australia in 2007.
The following cases were documented by doctors, medical papers, and filmmakers. Their diligent work allows us to be able to put them together and systematically analyze the mechanisms of injury associated with the HPV vaccines. ‘Our Paula Is Gone’Paula Aldea was a normal, healthy young girl. Since taking the HPV vaccine, she can no longer walk and now relies on a wheelchair. “Our Paula is gone,” her father said.
According to The Epoch Times documentary “Under the Skin,” on May 26, 2022, Paula received her first HPV vaccination. On June 25, she called her father at 10:25 a.m., crying at a bus stop and needing him to quickly come to get her—she could no longer feel her legs.
The pain in her back became unbearable, and then her back went numb. Paula and her father went straight to the emergency room and after some chiropractic exercises, she was told she’d be fine in a few hours and was sent home. At 3:00 p.m. her mother called her father and said, “Come home immediately. Paula doesn’t feel anything from her body anymore.”
“There was this pain. I think it was the worst pain I’ve ever had. And then this numbness—you just don’t realize it. You can’t walk, but you don’t think about it: What will the future be like? What will it be like now? Even when they said I had to stay in the hospital, I thought why?” said Paula.
Paula’s mother recalls, “When Paula was lying in her bed, the senior physician came and asked if she had had an infection recently. And we could deny that. She had neither a stomach bug nor a flu-like infection. Paula was always very healthy.”
“The next question was whether she had been vaccinated. And there it clicked—yes, she has been vaccinated. Everywhere we went to doctors, the second or third question was, ‘Did you have a vaccination recently?’” her mother said.
The damage has been officially recognized by authorities as caused by the HPV vaccine. Paula receives a monthly payment from welfare. Her inability to walk is likely caused by the severe attack of immune cells on the myelin layer of the spinal cord, which is an autoimmune response.
Paula is not a single case—she may even be the tip of the iceberg. There are numerous cases of disabilities, including an inability to walk or to see, following Gardasil injection. A 16-Year-Old American Girl Now BlindIn 2010, Dr. Frances DiMario Jr. from the pediatrics department at Connecticut Children’s Medical Center in Hartford, Connecticut, along with Drs. Mirna Hajjar and Thomas Ciesielski from the neurology department at Hartford Hospital, reported a case with a similar level of severity after HPV vaccination, in the Journal of Child Neurology.
Yuhong Dong Author (M.D., Ph.D.)
Yuhong Dong, M.D., Ph.D., is a senior medical columnist for The Epoch Times. She is a former senior medical scientific expert and pharmacovigilance leader at Novartis Headquarters in Switzerland, and was a Novartis award winner for four years. She has preclinical research experience in virology, immunology, oncology, neurology, and ophthalmology, and also has clinical experience in infectious disease and internal medicine. She earned her M.D. and a doctorate in infectious diseases at Beijing University in China.
|
|
FDA, CDC Hid Data on Spike in COVID Cases Among the Vaccinated: DocumentsBy Zachary Stieber
COVID-19 cases among vaccinated seniors soared in 2021, according to newly disclosed data that was acquired by U.S. health agencies but not presented to the public.
Humetrix Cloud Services was contracted by the U.S. military to analyze vaccine data. The company performed a fresh analysis as authorities considered in 2021 whether COVID-19 vaccine boosters were necessary amid studies finding waning vaccine effectiveness.
Humetrix researchers found that the proportion of total COVID-19 cases among the seniors was increasingly comprised of vaccinated people, according to the newly disclosed documents.
For the week ending on July 31, 2021, post-vaccination COVID-19 cases represented 73 percent of the cases among people 65 and older, the company found. The elderly were 80 percent fully vaccinated at the time.
Breakthrough infection rates were higher among those who were vaccinated early, the researchers found. They estimated that the rates were twice as high in those who had been vaccinated five to six months prior, when compared to people vaccinated three to four months before.
The breakthrough cases started in January 2021, according to the data.
Protection against hospitalization was also fading, researchers discovered. In the week ending on July 31, 2021, 63 percent of the COVID-19 hospitalizations in seniors were among the fully vaccinated, according to the documents. The same pattern of weaker protection among people who were vaccinated early was found.
It’s Really Happening: Vaccine and Mask Mandates, Contact-Tracing RETURN
Researchers calculated that the vaccine effectiveness (VE) against infection was just 33 percent while the effectiveness against hospitalization had dropped to 57 percent.
Seniors who previously had COVID-19 and recovered were more likely to avoid hospitalization, the researchers also found. Risk factors included serious underlying conditions such as obesity and being in the oldest age group, or older than 85.
The cohort analysis was completed on 20 million Medicare beneficiaries, including 5.6 million seniors who received a primary series of a COVID-19 vaccine.
“Our observational study VE findings show a very significant decrease in VE against infection and hospitalization in the Delta phase of the pandemic for individuals vaccinated with either the Pfizer or Moderna vaccine for those 5–6 months post vaccination vs. those 3–4 months post vaccination,” Dr. Bettina Experton, Humetrix’s president and CEO, said in a Sept. 15, 2021, email to top U.S. Food and Drug Administration (FDA) officials.
Humetrix also found that among the beneficiaries, there had been 133,000 cases, 27,000 hospitalizations, and 8,300 intensive care admissions among the fully vaccinated since the start of the COVID-19 pandemic.
Dr. Experton disclosed that Humetrix shared the data with the U.S. Centers for Disease Control and Prevention (CDC) in August 2021.
“It would have been nice to know [the military] was conducting this prior to now. Also might have been nice for CDC to share the data,” Dr. Peter Marks, one of the FDA officials, told colleagues in response.
“This is more worrisome than the other data we have in my opinion,” Dr. Janet Woodcock, the FDA’s acting commissioner at the time, said in reply.
The presentation and emails were obtained by the Informed Consent Action Network, a nonprofit that seeks to provide transparency around medical issues, through the Freedom of Information Act (FOIA).
“It is hard to see this as anything other than a failure of our health authorities to assess, share, make public, and act upon valuable, real-world data in the midst of a so-called pandemic,” Del Bigtree, founder of the network, told The Epoch Times via email. “And without FOIA, the public likely would never be made aware of these failures which, of course, allows them to be perpetrated again and again.”
The FDA and CDC declined to comment. Dr. Francis Collins, the director of the U.S. National Institutes of Health at the time, wrote in a separate email obtained through FOIA that the results of the study provided “pretty compelling evidence that VE is falling 5–6 months post vaccination for both infection and hospitalization for those over 65.”
He added, “Even for those 3–4 months out there is a trend toward worsening VE.” The CDC, FDA, and National Institutes of Health did not share the data with the public as they considered whether to clear and recommend COVID-19 vaccine boosters.
The CDC held a meeting with its vaccine advisers on Aug. 30, 2021. During the meeting, CDC officials went over emerging data on waning vaccine effectiveness. But the military study was not included.
The FDA held a similar meeting on Sept. 17, 2021. The CDC participated. The Humetrix analysis was also not presented during that meeting.
Both agencies have aggressively promoted COVID-19 vaccines throughout the pandemic, including hyping them as strongly protective against severe disease even after their own data have suggested that is not the case.
The CDC did present (pdf) data from COVID-NET, one of its systems, that showed effectiveness against COVID-19-associated hospitalization was falling among the elderly since the emergence of the Delta variant but that data still showed 80 percent effectiveness.
The presentation also included data from outside researchers and Israel that estimated the protection during the Delta era against infection ranged from 39 percent to 84 percent and that the effectiveness against hospitalization ranged from 75 to 95 percent.
The FDA ended up clearing a Pfizer booster for many Americans. The CDC advised most people to receive it. The agencies later expanded booster clearance and recommendations to virtually all Americans aged 5 and older, with Moderna’s shot as another option. Authorities have since replaced the old shots due to their lack of durability, and are preparing to roll out another slate of shots this fall.
Zachary Stieber Zachary Stieber is a senior reporter for The Epoch Times based in Maryland. He covers U.S. and world news. |
|
Forensic Analysis of Deaths in Pfizer’s Early mRNA Vaccine Trial Found Significant InconsistenciesResearchers are calling into question Pfizer’s early trial data on its original COVID-19 vaccine after a forensic analysis revealed significant problems.By Megan Redshaw
A group of researchers are calling into question Pfizer’s and BioNTech’s early trial data on its original COVID-19 vaccine after a forensic analysis revealed significant inconsistencies between data in the companies’ six-month interim report and publications authored by Pfizer/BioNTech trial site administrators.
The preprint, published on Sept. 4, showed trial subjects vaccinated with Pfizer’s COVID-19 vaccine experienced a 3.7 times increase in cardiovascular deaths compared to placebo controls—a “significant adverse event signal” not disclosed by Pfizer when the vaccine was authorized for emergency use. In addition, the analysis found numerous instances where Pfizer/BioNTech attributed potential vaccine-associated deaths to other causes and undermined vaccine safety data. Clinical Trial ‘Cause of Death’ Unsupported by DocumentationResearchers from the DailyClout Pfizer/BioNTech Documents Investigations Team assessed data from Pfizer’s original phase two/three clinical trial involving 44,060 subjects equally divided into two groups. One group received a dose of Pfizer’s COVID-19 vaccine, and the other received a placebo. As part of their analysis, researchers reviewed the cause of death forms (CRFs) of 38 trial subjects who died during the study period from July 27, 2020, to March 13, 2021, the end date of the clinical trial.
They found that 14 of the 38 deaths—more than one-third of deaths—resulted from cardiovascular events, accounting for the difference between the 21 deaths in the vaccination arm compared to the 17 deaths in the placebo arm. In numerous cases, researchers found that documentation did not support the cause of death diagnosis or allow one to rule out the possibility of a cardiovascular event with an autopsy.
“In general, our review of the CRFs found them to be lacking in detail and extremely difficult to interpret and develop a good timeline of events,” researchers wrote. “Often, a subject’s pre-trial clinical history was absent. Absent also were results of the extensive array of medical testing carried out at the pre-trial screening and at other regularly scheduled visits.”
Absent test results included complete blood counts, metabolic tests, pregnancy tests, COVID-19 tests, a comprehensive list of active medications, and other tests that would have provided clarity on a subject’s overall health. Although more detailed clinical data on the trial subjects exists, the researchers said it is being withheld. Given the limitations of what Pfizer provided, the researchers said the information in the CRFs was often insufficient to support the investigator’s conclusions regarding the cause of death.
The researchers also noted frequent communications between Pfizer/BioNTech physicians and trial site medical staff about the CRFs, some of which were over 400 to 900 pages. Pfizer Used Earlier Data Cutoff and Unblinded Control GroupAccording to the analysis, Pfizer excluded the 38 deaths from information provided to the U.S. Food and Drug Administration (FDA) during its December 2020 meeting where its vaccine advisory panel was considering whether to authorize the Pfizer/BioNTech vaccine for emergency use.
When Pfizer/BioNTech submitted its application for Emergency Use Authorization (EUA) on Nov. 20, 2020, to the FDA, the application described clinical trial results using a cutoff date of November 14, 2020, even though the end date of the trial was March 13, 2021. Researchers said the earlier cutoff date concealed mortality data from the clinical trial.
“Both Pfizer presenters and the FDA committee failed to ask for and review deaths that occurred in the clinical trial participants after the data cutoff. As a result, they missed a more than three-fold increased risk of cardiovascular death with the Pfizer-BioNTech COVID-19 vaccine,” cardiologist Dr. Peter McCullough told The Epoch Times in an email.
“If the FDA presentation with core slides had been presented with accurate, updated data, the Pfizer COVID-19 vaccine should not have been approved because of safety concerns,” he added.
Twenty weeks into the clinical trial on Dec. 11, 2020, Pfizer’s COVID-19 vaccine received EUA from the FDA, and the agency allowed Pfizer to unblind its control group. Unblinding occurs when study participants are told whether they received a vaccine or a placebo, and placebo subjects are permitted to get vaccinated. All but a few chose to receive the vaccine.
All subjects continued to be followed for 24 months and deaths were reported to Pfizer/BioNTech. Pfizer called the period from Dec. 11, 2020, to Jan. 24, 2021, the “open-label follow-up period” without explanation, and the period from Jan. 25, 2021, to the end date of the trial, March 13, 2021, as the cutoff date for the six-month interim report. According to the analysis, this made it easier to conceal deaths potentially linked to the vaccine.
A comparison of the number of deaths during the 33-week study period found no considerable difference between the deaths in the vaccinated versus the placebo groups for the first 20 weeks. After week 20, when participants in the placebo group were unblinded and vaccinated, deaths among the remaining unvaccinated cohort of this group slowed and then plateaued, while deaths in vaccinated subjects continued at the same rate. These inconsistencies were not explained by Pfizer/BioNTech or reported to the FDA, according to the analysis. Vaccinated Placebo Group Death Cases Used to Obscure Trial DataDocuments obtained through the Freedom of Information Act (FOIA) show that 462 subjects (pdf) in the placebo group received a dose of Moderna’s COVID-19 vaccine, with deaths reported attributed to the unvaccinated control group, and the analysis identified numerous instances where Pfizer/BioNTech undermined potential vaccine-related deaths or used complex terms to obscure trial data.
For example, a 65-year-old male with a medical history of pulmonary fibrosis and hypertension was in the trial’s placebo arm. He received doses 1 and 2 of the placebo on Sept. 30, 2020, and Oct. 21, 2020, respectively. After Pfizer/BioNTech unblinded the trial, he received his first dose of Moderna’s COVID-19 vaccine on Dec. 23, 2020. Five days later, on Dec. 31, 2021, he reported symptoms of COVID-19 and was admitted to the hospital.
While hospitalized, he became hypoxic and was intubated. Efforts to treat him failed, and he died on Jan. 11, 2021. Pfizer’s six-month interim report lists the subject as a “discontinued subject” and classified the death as a placebo death with COVID-19 as the secondary cause of death. The researchers said the subject should have been discontinued from the clinical trial entirely because he received a “non-study COVID-19 vaccine.”
Another trial subject, a 53-year-old male with a history of chronic obstructive pulmonary disease and “stress-related myocardial infarction,” died suddenly from “cardiopulmonary arrest” less than two months after receiving his second dose of Pfizer’s COVID-19 vaccine. According to the analysis, the trial site’s medical monitor listed the cause of death as “cardiopulmonary arrest related to myocardial infarction.” Days later, Pfizer/BioNTech told the trial site that multiple causes of death could not be entered on the CRF and requested that “related to myocardial infarction” be deleted.
When the medical monitor wouldn’t alter the entry’s wording, Pfizer/BioNTech overrode the trial site and changed the cause of death to “cardiopulmonary arrest,” omitting “myocardial infarction” as a secondary cause of death. Pfizer/BioNTech did not explain why a specific diagnosis of a serious adverse event was later changed to something undefined.
Another vaccine subject died within three days of receiving his first Pfizer vaccine dose. The medical examiner attributed the death to the progression of atherosclerotic disease, and Pfizer listed the cause of death in its six-month interim report as “atherosclerosis.”
However, atherosclerosis was not documented in the subject’s CRF as a comorbidity of the patient, nor did the subject’s CRF include the pre-screening portion of comorbidities that would have shown whether the subject had a history of atherosclerosis. Furthermore, an autopsy would have confirmed whether the subject died from atherosclerosis, but autopsy results were unavailable. The subject’s death was attributed to an underlying disease, yet the researchers said there is “no basis for ascribing the subject’s death to advanced atherosclerosis or concluding that the death was unrelated to the vaccine” when the subject died “within a day or two” of vaccination.
Another subject died 76 days after receiving the first placebo dose. The primary cause of death was first listed as diabetes mellitus based on the subject’s medical history. Yet the diagnosis was revised several times, despite the “presence of very high blood glucose levels,” until COVID-19 pneumonia was listed as the secondary cause of death. In addition, the subject was HIV positive with an HIV RNA load over the acceptable limit for inclusion in the trial.
“The FDA should review these data immediately in addition to the mounting safety data and peer-reviewed manuscripts on vaccine injuries, disabilities, and deaths and move swiftly to remove all COVID-19 vaccines from the market,” Dr. McCullough said. FDA and Pfizer Attempted to Hide Health Outcomes of Trial Participants: Preprint ResearchersWhen Pfizer/BioNTech filed its EUA in November 2020, the FDA didn’t make the application containing clinical data available on its website for the general public or the medical community to evaluate until Dec. 11, 2020. Although an article was published on Dec. 10, 2020, in The New England Journal of Medicine disclosing the interim results of the trial, it was authored by the trial site administrators who were “intimately aware of the trial’s findings,” researchers said.
The following year, in September 2021—after the Pfizer/BioNTech vaccine had received EUA—the same trial site administrators published another paper in The New England Journal of Medicine on the safety and efficacy of Pfizer’s COVID-19 vaccine through six months.
With the “knowledge and approval” of the FDA, the preprint researchers said Pfizer and the FDA had no plans to disclose the clinical trial data that formed the basis of EUA for the Pfizer/BioNTech vaccine for 75 years, including the health outcomes of the 44,060 subjects who participated in the original trial. It wasn’t until the Public Health and Medical Professionals for Transparency filed a FOIA lawsuit to obtain the original clinical trial data involved in the licensing of Pfizer/BioNTech’s Comirnaty vaccine that data was made available and the problems with the initial clinical trial were revealed.
Release of the data to the Public Health and Medical Professionals for Transparency site began early in June 2022 and was projected to take eight months to complete. They have taken much longer than estimated and documents continue to be downloaded.
“Had it not been for the successful court case brought by the Public Health and Medical Professionals for Transparency, no one outside of the Pfizer and BioNTech corporations would have had the opportunity to investigate the original data generated by this clinical trial and none of the discrepancies reported here would have been revealed,” they added.
The researchers said their analysis provides evidence the decision to authorize the Pfizer COVID-19 vaccine as a safe and effective means of controlling the pandemic was not an “informed decision based on an unbiased, thorough, and transparent evaluation of the evidence.”
Despite early warning signals and other reported adverse events in the post-marketing of mRNA vaccines, the Pfizer vaccine has not been removed from the market and has been approved for the nation’s youngest children. At the very least, the researchers said they hope their analysis will inform physicians and other medical professionals of the dangers of the mRNA vaccines so that they can better advise their patients on the personal risks compared with the benefits of getting vaccinated. “This would return healthcare decisions back to individuals and their medical providers where it belongs.”
The Epoch Times has contacted both Pfizer and the FDA for comment and has not yet received a response. Author (J.D.) Megan Redshaw is an attorney and investigative journalist with a background in political science. She is also a traditional naturopath with additional certifications in nutrition and exercise science. |
Medical Examiner’s Office source: Only 1 to 2 percent of ‘COVID deaths’ were really COVIDBy Selwyn Duke
“Only one to two percent” of deaths officially labeled as caused by COVID actually were induced by the disease. The rest were labeled as COVID but actually had other causes.
So said an individual I spoke to recently, who I’ll keep anonymous, about the deceased people processed by this individual’s medical examiner’s office. I won’t reveal much about this person, who I’ll call “ME,” except to say that ME is highly trained and qualified and works at a major medical examiner’s office in New York State.
ME’s information is not revelatory. We’ve heard from many sources that COVID numbers have been inflated. Personally speaking, I also talked a couple of years ago to an employee at a NY hospital who told me, casually and as a matter of course, “They’re lumping all the flu cases in with COVID.” But it’s especially noteworthy and newsworthy when the information comes from someone such as ME, who’s highly trained, in a position to know and who reveals such striking numbers.
I pressed ME on his (I’ll use the masculine pronoun generically here; this doesn’t imply that ME is male or not so) claim. “You’re not exaggerating?” I asked. ME confidently reiterated his assertion: Many deaths his office evaluated were attributed to COVID — but “only one to two percent” actually were.
What were the real causes? ME mentioned ischemia, myocardial infarction (heart attack) and complications from diabetes as major culprits. He also said that there were a large number of suicides — presumably another negative secondary effect of the lockdowns and other irrational COVID policies — though these were not labeled as COVID deaths at his office.
ME did state, however, that sometimes a person will have died from something wholly unrelated to COVID — he mentioned a motorcycle accident case as an example — and his office will list the decedent as having been “COVID positive” (not a COVID death, though), even though he wasn’t, because this would enable the deceased’s family to receive financial aid for the funeral.
Related to this, ME mentioned how not only were hospitals getting more money from the government if a patient was labeled COVID-positive, but that he believed funeral homes were also receiving funds for processing COVID-positive decedents, though he was unsure on this point.
Obviously, however, the monetary carrot will always corrupt a system: As is said, what you fund, you get more of.
ME doesn’t approve of the dishonesty at his office, of the gross manipulation of COVID numbers. But ME also mentioned that his role isn’t to sign the death certificates; it’s to provide the office itself with accurate information derived from his evaluation of decedents. As for the people who run things at this medical examiner’s office, ME wasn’t very impressed, describing them as fools (though ME used a different but synonymous term).
Lastly, ME mentioned something I’ve long pointed out: While with the flu, for example, the mortality counter is reset every year, this isn’t done with COVID. Rather, authorities keep a running count, continually adding on to the previous years’ numbers, so that the disease’s mortality appears especially frightening.
So what are America’s actual COVID numbers? Can ME’s one-to-two-percent estimate be extrapolated to our whole country? We don’t know. What’s for certain is that COVID has been grossly mismanaged and mischaracterized by people who would sententiously scold “Follow the science!” but were themselves following money and politics. In the process, this medical/scientific establishment has perhaps permanently discredited itself — and never was reputational destruction more richly deserved.
|
They control you by Fear Porn Propagandaby Tyler Durden, 01October2023 – https://www.zerohedge.com/political/climate-fear Authored by James Gorrie via The Epoch Times, The medical, media, and political elites’ focus has shifted from facts to fomenting and magnifying fear. In Franklin D. Roosevelt’s first inaugural address in 1933, the new president told a nation in the depths of the Great Depression that “the only thing we have to fear is fear itself.”
Those words were true and rightfully spoken at that time. Roosevelt knew that fear is a powerful emotion that limits our ability to reason, act wisely, and work together. It’s also an emotion that’s contagious and not easily diminished or dissipated.
The Power of Fear to Fragment SocietyUnfortunately, Roosevelt’s words are even more applicable today. On a personal level, decisions made under the emotional duress of fear are rarely the best ones and often the worst. Fear can bring out the best in us, but can often bring out the worst. That’s more likely to occur the more fragmented a society becomes. Fear among different groups of people creates an us-versus-them context in the minds of individuals, or even an “every-man-for-himself” attitude, which pits one group against another or even each of us against each other.
Now elevate that sense of fear to the level of the national electorate. A people or a nation that’s paralyzed with fear makes rash decisions based on their fears of what could happen, not necessarily what the current situation truly is. When that happens, a society can quickly degenerate, where our base instincts determine our behavior in a law-of-the-jungle social environment.
Roosevelt knew this, as do our leaders today. The difference is that today, rather than seeking to dispel fear, our political and media elites create it, expand it, and revel in it. Rather than promote hope and strength of character in us, in a Roosevelt- or even a Reagan-like fashion, they traffic in fear and its fellow traveler social division in order to fragment our society.
It’s the old but effective divide-and-conquer strategy, and sadly, it works far too well. The mechanism for divide and conquer is the constant drumbeat of the Big Lie, which is also a tried and true method for controlling society. It was first practiced and perfected by Joseph Goebbels in Nazi Germany using the mass media, but has been successfully used by the USSR and every other communist and dictatorial regime in the world since the 1930s. Social Media Is Magnitudes More Powerful Than Legacy MediaThe difference today is the massive and pervasive presence of social media. Its reach and social saturation throughout society are magnitudes greater than have ever been possible before. What’s more, our political and media elites create and exaggerate fear without even mentioning the word. “Fear” is driven into our collective psyches under the guise of our government keeping us “safe,” while demonizing anyone who challenges that narrative.
The repetition by the media and the pharmaceutical industry of how to stay safe from COVID-19 always involves more drugs and less freedom. That’s by design. The elites that run society know that once enough of our friends, neighbors, coworkers, and others with whom we interact become more fearful than rational, they’re easily manipulated and divided into confrontational groups.
Does that sound like a conspiracy theory? Yes, it probably does, but it’s also how the Stasi, the East German security agency, turned virtually every neighbor into an informant. The result was that people were fearful of doing anything that could be construed as being against the communist East German government. In light of what we’ve been through the last three years—and what looks to be on the horizon—the conspiracy theory accusation has lost its sting. From Conspiracy Theory to FactRecall, for example, how those who received the COVID-19 vaccine turned against those who remained unvaccinated. The contrast and social division couldn’t have been clearer or more deliberate. Vaccinated people were characterized by the media and government agency spokespeople as selfless, smarter, and better human beings than those who refused the vaccine.
On the flip side, the “anti-vaxxers,” as they came to be called, were publicly derided by the medical, pharmaceutical, media, and government elites. They were accused of being low-intelligence conspiracy theory nuts who wouldn’t or couldn’t “follow the science,” even when they followed the science from experts such as Robert Malone, one of the inventors of the mRNA technology, and other medical doctors in Europe and Asia, including former Pfizer Vice President Dr. Michael Yeadon, all of whom were de-platformed from mainstream media and social media.
In fact, any “alternative” remedy to the experimental and highly dangerous mRNA vaccines, such as ivermectin, was summarily dismissed, even though nations that used ivermectin had the lowest mortality rates. As noted above, many media personalities and even medical experts with contrary opinions were silenced, shamed, and shunted into professional oblivion, being substituted by compliant replacements. That practice continues to this day, with Russell Brand being the latest example of being de-monetized by YouTube.
In light of vaccine injuries and deaths, and the staggering profits that vaccines have delivered to the pharmaceutical industry, the number of people who believe the mainstream media, the government, and in the vaccines, is much smaller today than three years ago.
Conspiracy theory narratives have become conspiracy facts. The Endgame of FearSo, what’s the endgame of promoting and enforcing a climate of fear throughout society?
It’s simple. Fearful people are far more compliant and, therefore, are easily controlled, pacified, monitored, and dehumanized. Next thing you know, we’ll all be eating bugs and liking it.
The antidote to fear, of course, is freedom and access to real and contrary information so that each person can make up his or her own mind. The encouragement, enablement, and empowerment of private individuals to exercise informed judgment about their health and their livelihoods are also part of the solution. A vibrant, thinking, and active society of informed individuals isn’t nearly as vulnerable to the polarizing climate of fear our elites are foisting upon us. In short, to live in fear is to live in bondage. |
|
Israeli Ministry of Health Mask Fear Porn PropagandaJerusalemCats Comments: This is the only mask you need.  Friday the 13th Horror Movie, Jason Yoorhees  Friday the 13th Horror Movie, Jason Yoorhees From the propaganda site called Arutz 7
Is COVID coming back? Health Ministry recommends masksMinistry of Health recommends that people at high-risk use a mask in closed places to minimize the risk of infection.Israel National News
The Ministry of Health said on Tuesday evening that there is a moderate increase in the number of people hospitalized from coronavirus in Israel.
“The ministry constantly monitors the morbidity trends and variants of the coronavirus and, as of this moment, a moderate increase in the number of hospitalized patients is evident in Israel. Both in Israel and in the world, there are a number of variants that cause morbidity,” it said.
Ahead of the holidays and as a result of the increase in morbidity, the Ministry of Health recommends that if a person is in a high-risk group or wishes to reduce the risk of infection, use of a mask in closed places with many people is advised. It is also recommended that a mask be used when meeting with people who are in high-risk groups. The Ministry of Health stated that it is important for a patient with symptoms to remain in isolation until the symptoms pass, and added that if a sick person needs to go outside, it is recommended that he wear a mask.
It was also noted that “it is important to maintain awareness and be tested at home for early detection when there is a suspicion of illness. The ministry is preparing to provide dedicated vaccines against the new subvariants in the near future.”
|
|
CDC Data Show COVID Hospitalizations on the DeclineAfter multiple weeks of increasing COVID-19 hospital admissions, federal data shows that the figure is now falling.26September2023 Updated: 28September2023 https://www.theepochtimes.com/health/cda-data-show-covid-hospitalizations-on-the-decline-5499008
After multiple weeks of increasing COVID-19 hospital admissions, federal data show that the figure is now falling.
In the week ending Sept. 16, U.S. Centers for Disease Control and Prevention (CDC) data show hospitalizations are down 4.3 percent. The number had been increasing since July, although the CDC’s historical trends shows that hospitalization numbers were relatively low compared with previous increases in the virus—notably compared with a prior “surge” that occurred in the summer of 2022.
Meanwhile, the latest figures show that emergency department visits are down 19.3 percent and test positivity is down 1.6 percent. Deaths are up by about 12.5 percent, the data show, but that figure is also relatively low when compared with previous years.
The EG.5 variant, which has been dubbed Eris, accounts for about 24.5 percent of all cases, according to the CDC’s variant tracker. FL.1.5.1, known as Fornax, is estimated to be responsible for about 13.7 percent of COVID-19 infections, the CDC figures show.
About a month ago, amid a steady rise in hospitalizations, some health officials suggested that it doesn’t appear to be as bad as before.
“Looking at that graph [of] hospitalizations, even though it’s on an upward trend, that’s still lower than it was last year at this time,” Dr. John Segreti, an epidemiologist and the medical director of infection control and prevention at Rush University Medical Center in Chicago, told ABC News. “The fact that the numbers are going up fairly slowly, I think is a good sign.”<
Responding to the figures last month, Dr. Shira Doron, chief infection control officer for Tufts Medicine, said that the recent “upswing is not a surge; it’s not even a wave.”
“What we’re seeing is a very gradual and small upward trajectory of cases and hospitalizations, without deaths really going along, which is great news,” the doctor added.
Last week, the Biden administration announced it would use $600 million to produce new COVID-19 tests that it will send out for free to people who order them via the U.S. Postal Service.
Twelve manufacturers that employ hundreds of people in seven states from California to Maryland have been awarded funding and will produce 200 million over-the-counter tests to replenish federal stockpiles for government use, in addition to producing enough tests to meet demand for tests ordered online, the Department of Health and Human Services said.
Dawn O’Connell, assistant secretary for preparedness and response at HHS, said that though some portions of the public may be tired of the pandemic and its implications, at-home testing remains a key way to slow the spread of new cases.
“Whether or not people are done with it, we know the virus is there, we know that it’s circulating. We know, if past is prologue, it’ll circulate to a higher degree and spread, and cases will go up in the fall and winter seasons,” Ms. O’Connell said. “Anticipating that that would be true again, or something similar, we want to make sure the American people have these tools.”
Mandates?The publication of the new data comes after a handful of hospitals, county governments, and a small number of schools and colleges mandated mask requirements starting in August. The CDC and Food and Drug Administration (FDA) again recommended new COVID-19 booster shots for anyone aged six months and older earlier this month.
And several Bay Area health agencies in California announced last week that mandatory masking would return to hospitals and health care settings for the fall and winter months.  People, some still wearing masks, ride a subway in Brooklyn in New York City, on May 11, 2023. (Spencer Platt/Getty Images) Contra Costa, Sonoma, Alameda, and San Mateo counties issued mask orders for health care staff in hospitals and other care facilities. The orders start on Nov. 1 and last until April 30, 2024, officials said, citing recent increases in COVID-19, influenza, and other respiratory viruses that are typically commonplace during the colder months, according to statements and local media reports.
“Each year we see that higher rates of influenza, COVID-19 and other respiratory viruses that can cause severe respiratory infections occur annually between late fall and spring,” Dr. Karen Smith, the Sonoma County interim health officer, said in a statement.
Contra Costa Health Services CEO Anna Roth, meanwhile, the Northern California county’s board of supervisors last week that the mandate will be enacted, according to local media reports.
“We are issuing the health order today around masking for high-risk facilities, health care facilities specifically,” Ms. Roth stated, according to a local CBS affiliate station. “So again, masking in hospitals, masking in skilled nursing facilities, masking in high-risk facilities.”
Mask mandates have already been in effect at hospitals in San Francisco. The city is already enforcing year-round masking for health care staffers, visitors, and patients, reported the San Francisco Chronicle. Officials in Santa Clara County, which encompasses much of Silicon Valley, already set a mask mandate back in March.
Jack Phillips
|
|
Dear fully vaccinated: The newly approved COVID shot is NOT a booster – it is literally a new (untested) vaccine15September2023 // Ethan Huff // https://www.naturalnews.com/2023-09-15-new-covid-shot-not-booster-kathy-hochul.html
If you already previously got “vaccinated” and “boosted” for the Wuhan coronavirus (COVID-19), congratulations: you accomplished absolutely nothing except for the destruction of your immune system because the latest circulating COVID “variants” are no match for anything other than the newest COVID jabs to be approved by the U.S. Food and Drug Administration (FDA).
This is basically what New York Gov. Kathy Hochul told her constituents this week following the FDA’s decision to approve and emergency use authorize (EUA) the “updated” COVID jabs from Pfizer and Moderna.
According to Hochul, all previous COVID injections are ineffective against newer variants like Omicron XBB.1.5. As such, the fully vaccinated will need to head on down to the clinic once again to take these latest Big Pharma shots if they hope to stay protected this fall and winter.
“It is literally a new vaccine,” Hochul said, delivering that line in her best “valley girl” voice. “It is not a booster shot. It is not an enhancer. It is a new vaccine designed to attack the new variants.”
Put another way, Hochul is basically saying that Operation Warp Speed did nothing, and that now everyone must get jabbed once again if they wish to survive COVID 2.0.
(Related: Did you know that Kathy Hochul wants to ban gas stoves in the state of New York because of “global warming?”)
Hochul: Refusing to take newest COVID jabs means you’re selfishIf that message alone is not enough, Hochul went on to state that this is all no big deal because Americans have already been getting jabbed again and again since the beginning.
“We’ve done this since March 2020 – no reason to stop now,” Hochul said, trying to be funny. “Don’t think about just yourself.”
“Tell everybody: Don’t rely on the fact that you had a vaccine in the past – it will not help you this time around,” she further emphasized. “Even for healthy adults, COVID is serious – you don’t want to get it.”
In other words, do not be upset that you already took two, three, four, or even more COVID jabs because the government promised you would be protected, only to have that protection disappear in an instant because oopsie. No, you should instead just shut up, stop being selfish and just get jabbed again, according to Hochul.
Playing the part of bureaucrat doctor, even though she is barely qualified to run a hot dog cart, Hochul promised New Yorkers that if they will just agree to take this new shot, then that will be the end of getting COVID jabbed – for now, anyway.
“I will be getting my vaccine very soon,” Hochul promised unconvincingly. “This news is coming at a perfect time. My team just got off a call with the FDA confirming the COVID vaccine is on its way to New York.
“The updated vaccine guards against the newer COVID strains because it was built off the Omicron … variant – that’s what we’re calling it. It’s really a customized vaccine … We’re waiting to find out what age groups the FDA and CDC are recommending should get the shot … You only need one, no more double doses, and again, this will be starting here in New York on Friday.”
Hochul would end her propaganda speech by reiterating the same tired lie that “the vaccine has always been the best way to protect yourself and your community against COVID-19,” even though she said earlier in the speech that “the vaccine,” referring to the old vaccines, have failed.
Want to keep up with the latest news about what becomes of folks who take the newly approved COVID jabs from Pfizer and Moderna? You can do so at Vaccines.news.
Sources for this article include:
|
|
The Medical Industrial Complex is at it again
Mayo Clinic Nukes Hydroxychloroquine Information Page After People Take Noticeby Tyler Durden, 28September2023 – https://www.zerohedge.com/political/mayo-clinic-nukes-hydroxychloroquine-information-page-after-people-take-notice
One day after the Mayo Clinic’s endorsement of Hydroxychloroquine was highlighted for use in Covid-19 patients, they scrubbed the page and then blamed a 3rd party vendor for supplying the information.  Hydroxychloroquine
The original page read: “Hydroxychloroquine may be used to treat coronavirus (COVID-19) in certain hospitalized patients,” which was highlighted various people and oulets, including ZeroHedge, and former Trump official Peter Navarro.
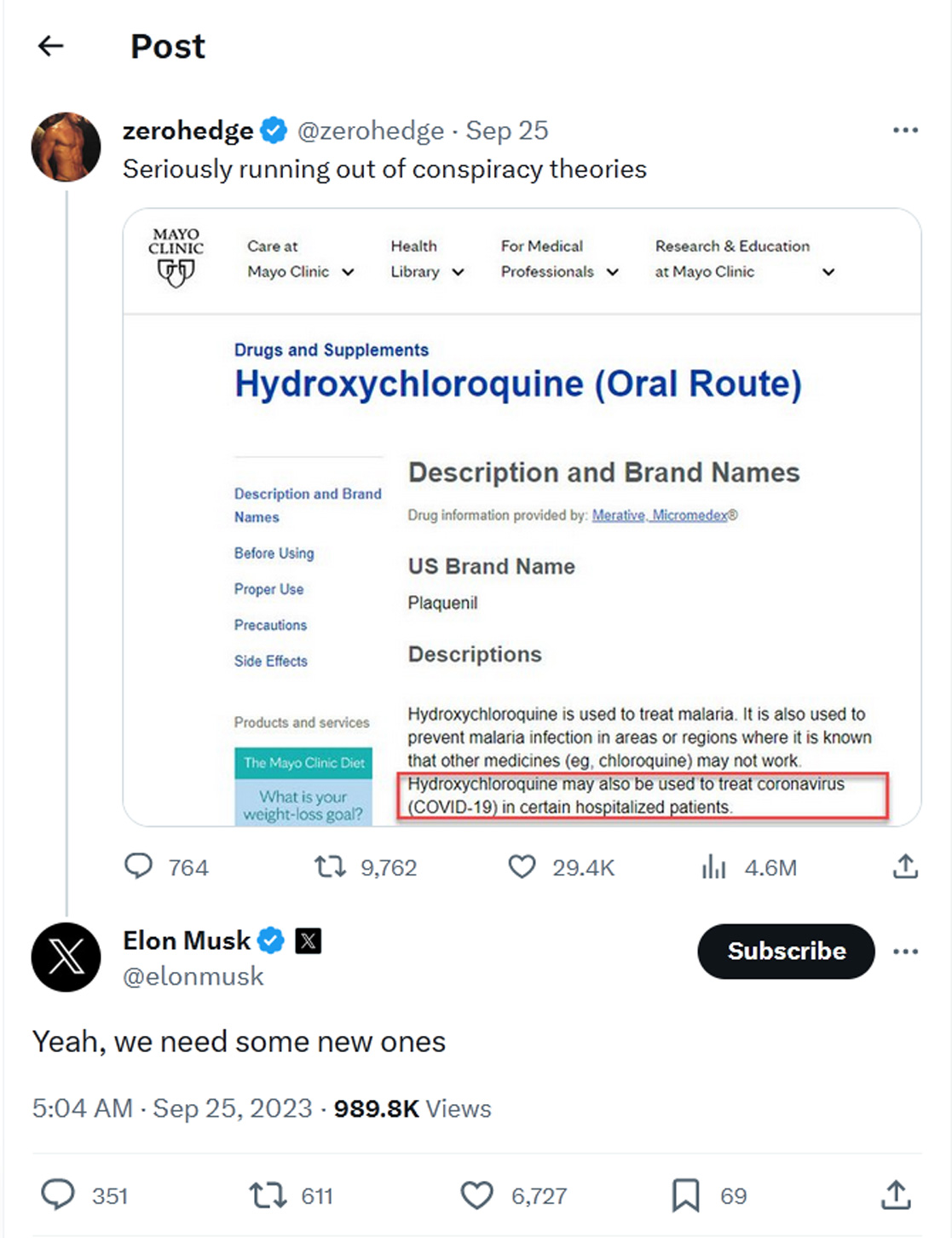 zerohedge-tweet-25September 2023-Seriously running out of conspiracy theories Now, the Mayo Clinic redirects people to a “safe” page.
Of course, pro-vax (we assume) outlets pounced on the fact that this information has been there since at least May of 2020.
Which means… by the transitive properties of woke outrage, the Mayo clinic has been spreading misinformation for three years? Cancel them!
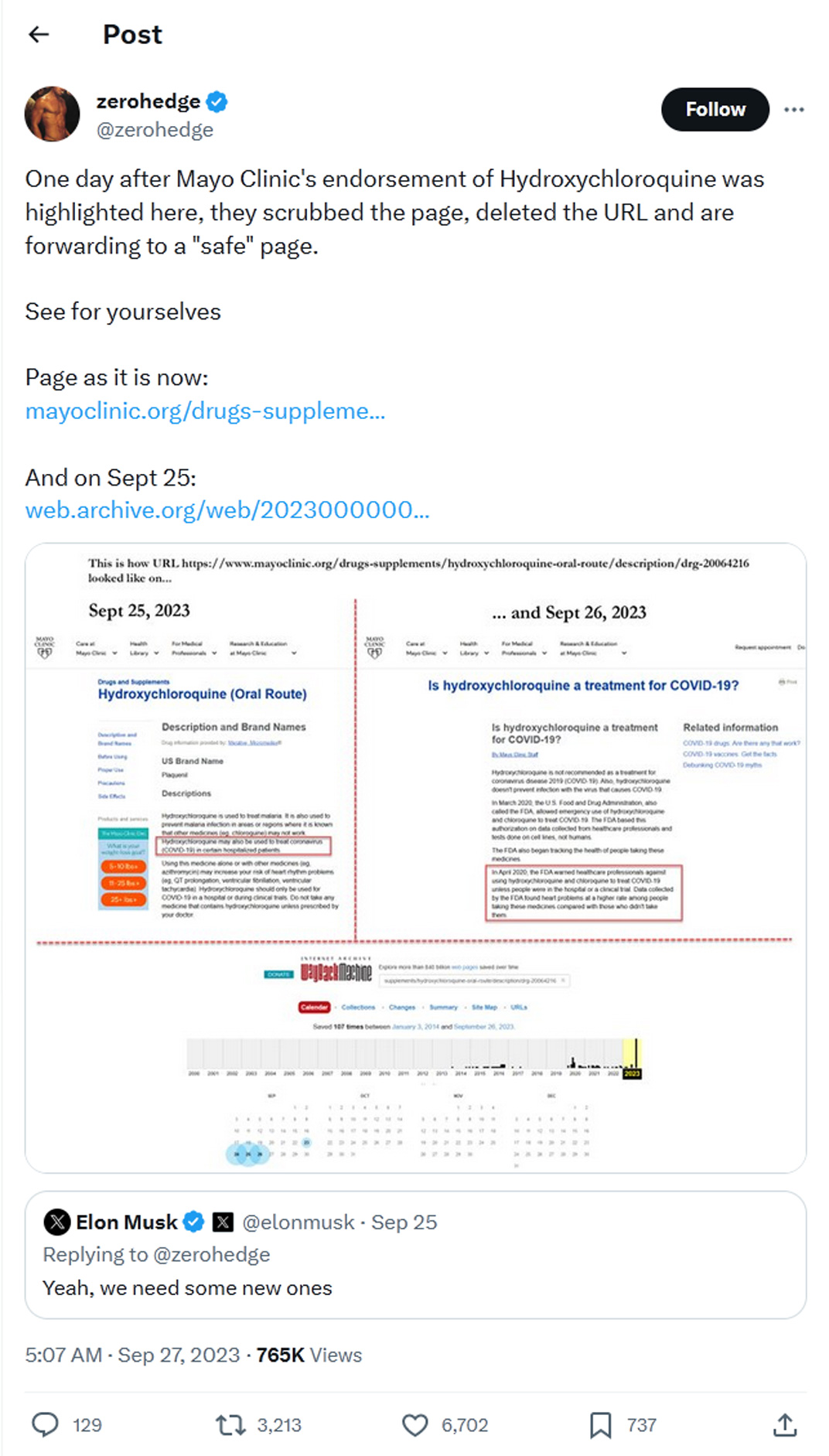 One day after Mayo Clinic’s endorsement of Hydroxychloroquine was highlighted here, they scrubbed the page
Meanwhile, an analysis of dozens of studies on Hydroxychloroquine and COVID-19 reveals a 72% lower mortality risk when taken early, and a 41% lower mortality risk when given early into hospitalization (when both HCQ and Ivermectin are known to be less effective vs. at first symptoms). 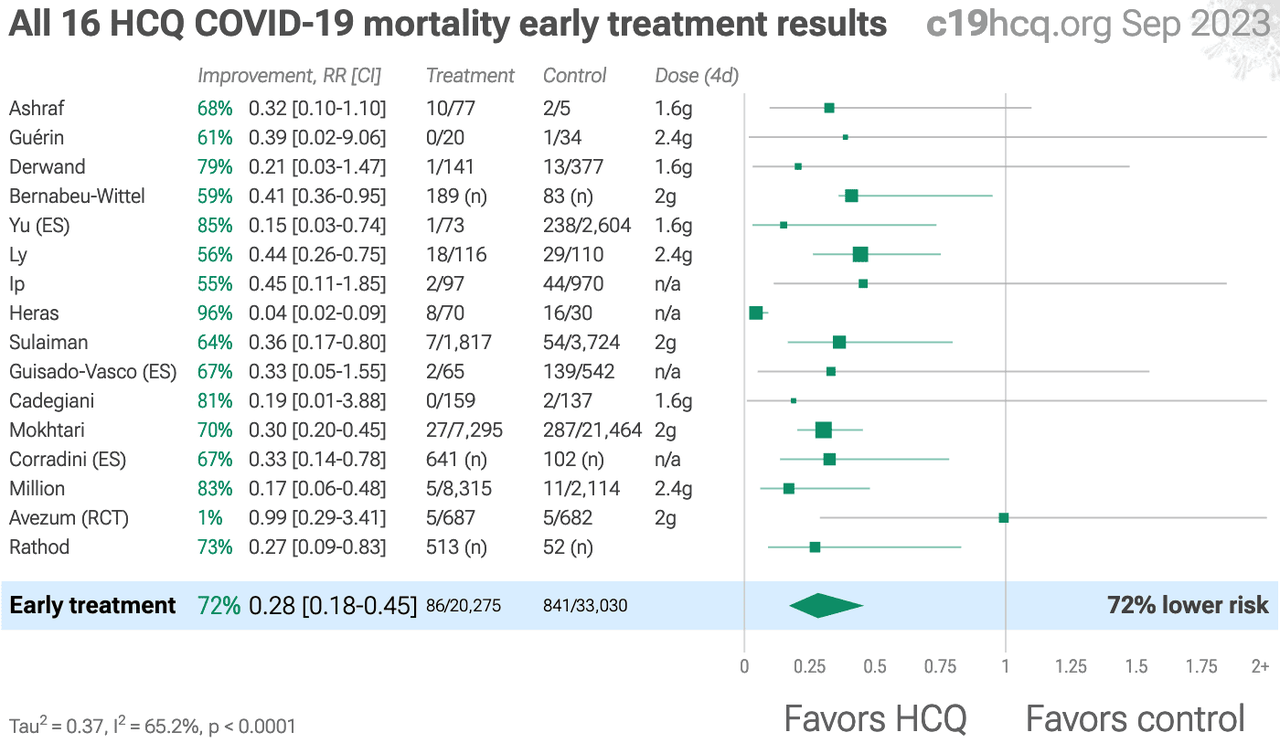 All 16 HCQ COVID-19 mortality early treatment results
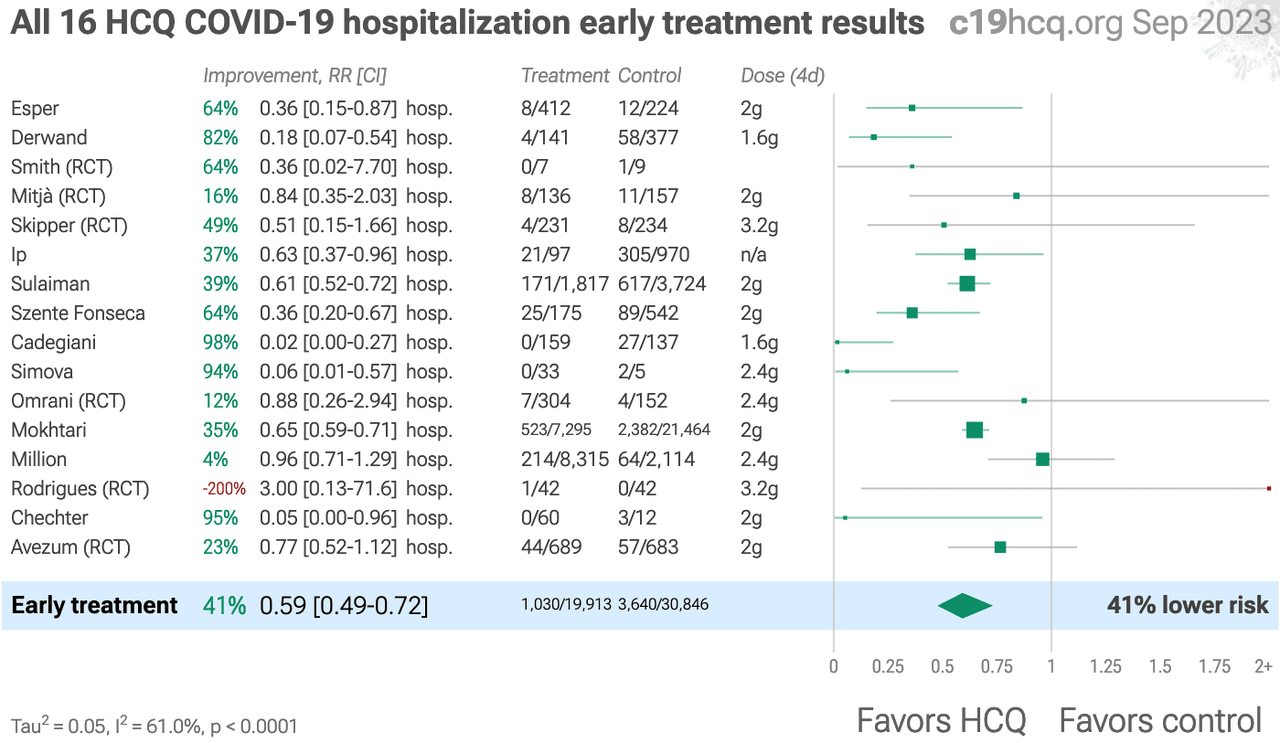 All 16 HCQ COVID-19 hospitalization early treatment results
See the full study results here… |